
Translate this page into:
Dermoscopy of nevoid hyperkeratosis of the nipple and/or areola in Fitzpatrick skin type IV
*Corresponding author: Payal Chauhan, Department of Dermatology, Venereology and Leprology, All India Institute of Medical Sciences (AIIMS), Himachal Pradesh, India. chauhanpayal89@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chauhan P, Dhiman A, Daroach M. Dermoscopy of nevoid hyperkeratosis of the nipple and/or areola in Fitzpatrick skin type IV. J Cutan Aesthet Surg. 2024;17:332-4. doi: 10.4103/JCAS.JCAS_175_22
Dear Editor,
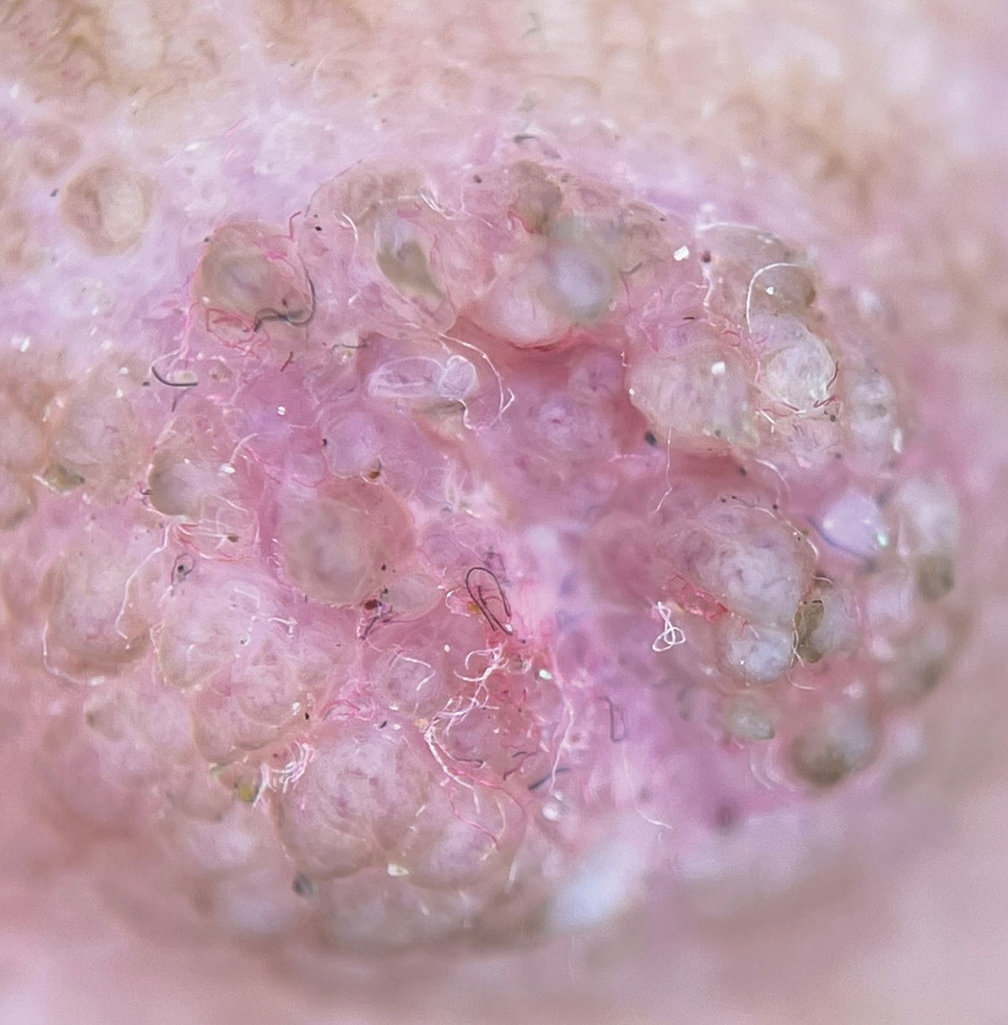
A 16-year-old female Fitzpatrick skin type IV presented with a history of non-itchy, painless, brownish lesion on both nipple which started around 6 years back after the patient attained puberty. Upon clinical examination, there were multiple, irregular, skin-colored projections, few with overlying adherent brownish to hyperpigmented crust present on both nipples [Figure 1a]. Dermoscopy (DermLite DL4; 3Gen; San Juan Capistrano, California, USA, noncontact polarized mode, 10x magnification, images capture with Dermlite adapter for iPhone 12 pro max) demonstrated multiple papillated growths having overlying linear curved vessels and linear vessels with branches, and white clods. Yellow-brown scales and crust along with peripheral brown pigmentation were also appreciated [Figure 1b]. Histopathological examination of the patient was done and revealed acanthosis, keratin plugging, papillomatosis, anastomosis of rete ridges with vascular dilation and fibrosis in dermis [Figure 2a and b]. A final diagnosis of nevoid hyperkeratosis of the nipple and/or areola (NHNA) Type 3 was made after clinicopathological correlation. The patient was started on topical mometasone furoate cream 0.1% and urea-based moisturizer with considerable improvement after 1 month [Figure 3].

- (a) Hyperkeratotic, papillated projections few with overlying adherent brownish to hyperpigmented crust. (b) Dermoscopic examination showing multiple papillated growths (blue arrow) having overlying curved vessels and linear vessels with branches (yellow arrow), white clods (in a circle). Yellow-brown scales and crust (red arrow) along with a peripheral brown pigmentation (black star) was also appreciated.
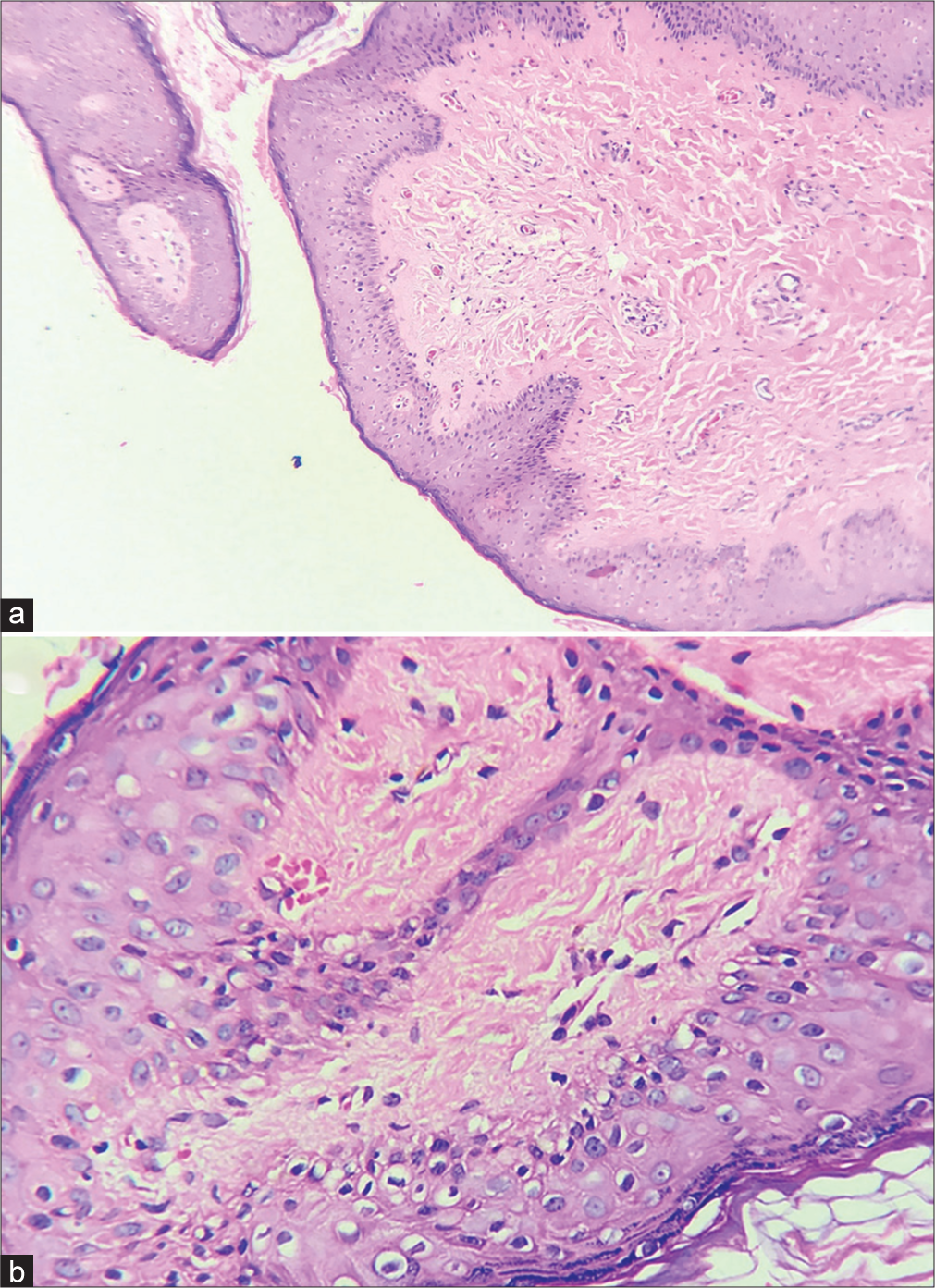
- (a) Histopathological examination showed epidermal acanthosis, keratin plugging, papillomatosis, anastomosis of rete ridges along with dilatation of vessels and fibrosis present in the dermis (H&E, 10×). (b) Presence of anastomosis of rete ridges and dilation of dermal vasculature appreciated better in higher power (H&E, 40×). H&E: Hematoxylin and eosin.
- Post-treatment dermoscopic image showing decrease in papillated growths, reduction in vasculature and white clods.
NHNA is a rare skin disease with an unknown etiology presents as diffuse, hyperpigmented, verrucous asymptomatic plaques covering nipple, areola or both.1 Despite being benign, it can be upsetting for the patients because of its appearance. Levy-Frenckel divided it into three categories in 1938.2
Type 1: Associated with an epidermal nevus
Type 2: Linked to a number of dermatoses, including Darier disease, chronic eczema, acanthosis nigricans, and cutaneous T-cell lymphoma
Type 3: Isolated, etiologically undetermined
NHNA is viewed as a diagnosis of exclusion and its differentials include erosive adenomatosis, seborrheic keratosis, verrucous epidermal nevus, and viral wart.3 Dermoscopy of differentials of NHNA is summarized in Table 1.3,4 Dermoscopic appearance of multiple papillae having overlying vessels along with white globules, in absence of other findings like ridges, comedo-like openings, fissures, brown globules, or cobblestone-like appearance help differentiate NHNA from its clinical mimickers like seborrheic keratoses and verrucous epidermal nevus. Viral warts on dermoscopy show closely grouped papillae with central vessel, the papillae are surrounded by a whitish halo which was not seen in the present case of NHNA. Dermoscopy helps differentiate erosive adenomatosis of nipple from NHNA by displaying red globules, red structureless areas, pink-white clouds on a reddish-white/red background in the former.
| Erosive adenomatosis of nipple | Whitish/yellowish hyperkeratosis and sparse dotted vessels on a pinkish background, cherry -red dotted and linear vessels on a pinkish background or increased red serpiginous and annular structures |
| Seborrheic keratosis | Fissures, ridges, comedo-like openings, milia like cyst |
| VEN | Brown circles having hyperchromic brown edge surrounding a hypochromic area, fissures, milia-like cysts, brown globules, or cobblestone-like appearance |
| Verruca vulgaris | Densely packed papillae, each containing a central red dot or loop, which is surrounded by whitish halo |
| Present case of NHNA | Multiple papillation with overlying vessels, white clods, peripheral brown pigmentation, and scales/crusts |
NHNA: Nevoid hyperkeratosis of the nipple and/or areola, VEN: Verrucous epidermal nevus
Dermoscopic findings of NHNA have been described in only a handful of cases with a papillomatous surface having pink homogenous areas, red dots, erosions, and pigment network being the predominant findings reported.3 Upon dermoscopic histological correlation, papillated growths correspond to underlying epidermal papillomatosis, white dots reflect keratin plugging and/or dermal fibrosis, and vessels are secondary to dermal vasodilation.
In a recent report of NHNA associated with darier disease, a central crater with an angulated border, filled with yellow to yellowish-brown keratotic plug, and surrounding white radial streaks were seen on dermoscopy.5
To the best of our knowledge, our case is the first report describing dermoscopic findings with NHNA Type 3 in skin of color. Given the sensitive location, most patients with dermatoses of nipple/areola complex refuse to dermoscopy of NHNA, which can serve as a rapid, noninvasive modality under these constraining circumstances.
To conclude, dermoscopy of NHNA shows multiple papillation with overlying vessels, white clods, peripheral pigmentation, and scales/crusts and more studies are needed in this field to validate findings of the present case.
Authors’ contributions
Payal Chauhan: Concepts, design, definition of intellectual content, literature search, manuscript preparation, manuscript editing, manuscript review. Avita Dhiman: Concepts, design, definition of intellectual content, literature search, manuscript preparation, manuscript editing, manuscript review. Manju Daroach: Concepts, design, definition of intellectual content, literature search, manuscript preparation, manuscript editing, manuscript review.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Dermoscopic features of nevoid hyperkeratosis of the nipple and areola. Dermatol Pract Concept. 2022;12:e2022003.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical approach for nevoid hyperkeratosis of the areola. J Cutan Aesthet Surg. 2012;5:40-2.
- [CrossRef] [PubMed] [Google Scholar]
- Nipple and areola lesions: Review of dermoscopy and reflectance confocal microscopy features. J Eur Acad Dermatol Venereol. 2019;33:1837-46.
- [CrossRef] [PubMed] [Google Scholar]
- Co-localization of verruca vulgaris with verrucous epidermal nevus: Role of dermoscopy in diagnosis. Clin Dermatol Rev. 2021;5:260-2.
- [CrossRef] [Google Scholar]
- Dermoscopy and histopathology of darier disease-associated nevoid hyperkeratosis of nipple and areola. Dermatol Pract Concept. 2021;11:e2021044.
- [CrossRef] [PubMed] [Google Scholar]




