
Translate this page into:
Dirty Papules and Plaques in Skin of Color: New Observations by Dermoscopic Dissection
Address for correspondence: Dr. Balachandra Suryakant Ankad, Department of Dermatology, S N Medical College, Bagalkot 587102, Karnataka, India. E-mail: drbsankad@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Context:
Confluent reticulated papillomatosis (CRP), terra-firme-forme-dermatitis (TFFD), and dermatitis neglecta (DN) are the benign, acquired conditions that present with dirty-looking hyperpigmented and hyperkeratosis lesions on neck, back, and truncal areas. They pose difficulty in diagnosis because of their clinical similarities and thereby in treatment approaches. Bedside test and histopathology is helpful in the diagnosis. Dermoscopy is utilized as an evidence-based diagnostic method.
Aims:
To evaluate and to compare the dermoscopic patterns among CRP, TFFD, and DN and to correlate them in terms of histopathological features.
Materials and Methods:
It was a cross-sectional observational study with a total of 62 patients, among whom 30 were CRP, 20 had TFFD, and 12 were diagnosed as DN. Clinical and dermoscopic evaluation was done in all patients, and histopathology was carried out in selective cases to confirm the diagnosis.
Results:
Global view of dermoscopy in CRP revealed a cerebriform pattern. The arrangement of pigment globules was characteristic in CRP, TFFD, and DN, giving a “cobblestone,” “mosaic,” and “cornflake-like” appearance, respectively. The color of the pigment globules was strikingly significant. Yellow globules were predominant in CRP and TFFD, having p values of 0.001 and 0.004, respectively. Scales were conspicuously present in CRP, with a statistically significant p value of 0.003. Focal white areas and hair changes were observed in CRP alone, whereas black dots were found only in TFFD.
Conclusion:
Dermoscopy acts as an in vivo and a noninvasive, rapid technique in the diagnosis of clinically look-alike conditions. It demonstrates characteristic features in CRP, TFFD, and DN. Thus, it is an evidence-based diagnostic method that assists the treating physician in daily clinical practice.
Keywords
Cobblestone
confluent reticulated papillomatosis
cornflake like
dermatitis neglecta
dermoscopy
dirty-looking
mosaic pattern
terra-firme-forme-dermatitis

INTRODUCTION
Hyperpigmentary skin lesions are the major bulk of cases attending dermatology outpatient departments. They cause cosmetic disfigurement with an immense psychosocial impact, especially in the Indian subcontinent. Dermoscopy is a noninvasive diagnostic method that has gained stupendous importance in the diagnosis of hyperpigmented lesions.[1] CRP is a benign and acquired dermatosis, which is characterized by dirty-looking hyperpigmented and hyperkeratotic lesions with confluence in the center and reticulation at the periphery. The most common sites are the upper back, neck, and chest. The CRP affects adolescents and adults.[2] TFFD, also known as Duncan’s dirty dermatosis, is an idiopathic and benign condition, which is typified by dirty-looking hyperkeratotic brown to black papules and plaques in the neck, upper extremities, and the trunk. It is seen in children and adults.[3] DN occurs due to a lack of cleanliness, resulting in the accumulation of keratin, dirt, and debris. Clinically, it presents with hyperpigmented and hyperkeratotic papules and plaques. It usually affects the patients with chronic disease and is accompanied by pain or immobility of a part, where the patient is unable to clean the part.[4]
CRP, TFFD, and DN mimic each other clinically by presenting with hyperkeratotic, brown, or black papules and plaques. These lesions are dirty-looking. Although soap water and alcohol swabbing would remove the lesions in DN and TFFD, respectively, clinically one cannot be assured about the diagnosis. The CRP requires skin biopsy for confirmation.[5] Hence, for skillful diagnosis, these lesions mandate a histopathological study. Dermoscopy plays an important role in the authentic conclusion of numerous malignant skin conditions as well as in many inflammatory and infectious diseases of the cutaneous system. This technique is of great benefit, especially in facial dermatosis where a skin biopsy would be denied by bountiful patients or in clinically look-alike conditions where histopathology would be challenging.[6] Dermoscopic analysis of CRP, TFFD, and DN in the literature is limited to case reports. Along these lines, hiatus in the comparative studies, which would highlight the dermoscopic distinction of these entities, is prominent. Here, we have attempted to evaluate the dermoscopic patterns CRP, TFFD, and DN in skin of color, and to distinguish each from the other. An explanation of the histopathological correlation of dermoscopic patterns is also analyzed.
MATERIALS AND METHODS
This cross-sectional observational study was conducted in a tertiary care hospital in southern India from December 2019 to December 2020. Ethical clearance was taken from the institute, and written informed consent was obtained from all study participants. All the patients with clinically suspected lesions of CRP, TFFD, and DN were included in the study. Demographic data in terms of age, sex, occupation, and duration of the lesions were recorded. Patients with prior treatment, either topical or systemic therapy, one month prior to the enrolment and lesions with secondary pyoderma were excluded from the study. After clinical examination, dermoscopy was performed with a handheld manual dermoscope (Illuco dermoscope) having 10 x magnification. Polarized mode with ultrasonography gel as an interface medium was employed. Dermoscopic images were captured and saved in a dedicated camera. Images were analyzed by one of the authors (BSA). The site of dermoscopic examination was marked as the site for skin biopsy. Swabbing with 70% alcohol and soap water was carried out in all the lesions. Potassium hydroxide (KOH) mount was done to know the associated pityriasis versicolor in all the cases. Histopathological evaluation was performed to confirm the clinical diagnosis in selected lesions of CRP, TFFD, and DN. The data were entered into a Microsoft excel sheet and were statistically analyzed using SPSS software version 19.0. Percentages were used for qualitative data, and Chi-square test was applied for differences in the proportions. A p value of less than 0.05 was considered as statistically significant.
RESULTS
Totally, 62 patients (40 male and 22 female subjects) were included in the study. CRP was present in 30 patients; 20 and 12 patients had TFFD and DN, respectively. The average age was 30 years in CRP (minimum 16 years and maximum 44 years), 25 years in TFFD (minimum 20 and maximum 30 years), and 35 years (minimum 10 and maximum 60 years). CRP was distributed in the neck and upper back whereas TFFD was recognized on the chest, trunk, and lower legs. DN was situated in the anterior neck and abdomen. KOH mount was negative in all the cases. Dermoscopically, CRP showed, in global view, a brownish ridge and a whitish fissure pattern, giving a “cerebriform” pattern. In contrast, no definitive pattern was noted in both TFFD and DN. However, pigment globules on the ridges in CRP were in a “cobblestone” pattern [Figures 1,2,3–4]; however, in TFFD [Figures 5,6,7,8–9] and DN [Figures 10,11,12–13], globules were in “mosaic” and “cornflake-like” patterns, respectively. Interestingly, follicular change and focal white areas were detected in CRP alone. Follicular changes included broken hairs and V-hairs (two hairs emerging from a single follicle). Two cases of CRP revealed grayish-black pigment globules. Scales were found in all three conditions. They were predominant in CRP (100%) and were in a declining rhythm in TFFD (75%) and DN (50%). Comparative statistical analysis of scales using the Chi-square test conceded a highly significant p-value of 0.003. The color of pigment globules varied in each condition. The predominant color of pigment globules was brown, yellow, and black, respectively, in CRP, TFFD, and DN. However, the three colors mentioned were illustrated in all conditions with a variable degree, except for CRP wherein yellow color was not observed. The brown pigment globule was significantly associated with CRP (p value of 0.001). In the same line, yellow or the yellowish-brown pigment globule was prominent in TFFD with a P-value of 0.004. Black dots were observed only in TFFD. Salient dermoscopic features and their comparative analysis are depicted in Tables 1 and 2, respectively. Histopathological features were consistent with CRP [Figure 14], TFFD [Figure 15], and DN [Figure 16].
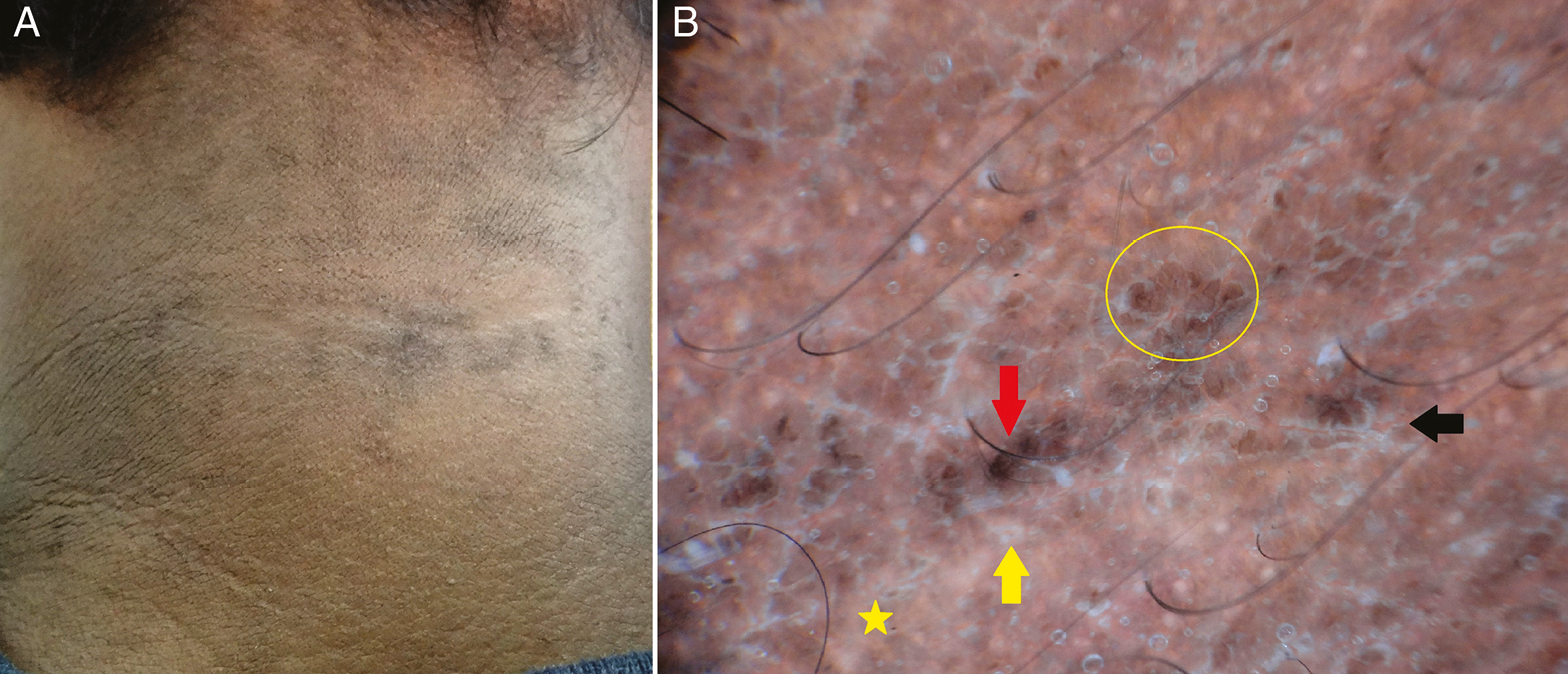
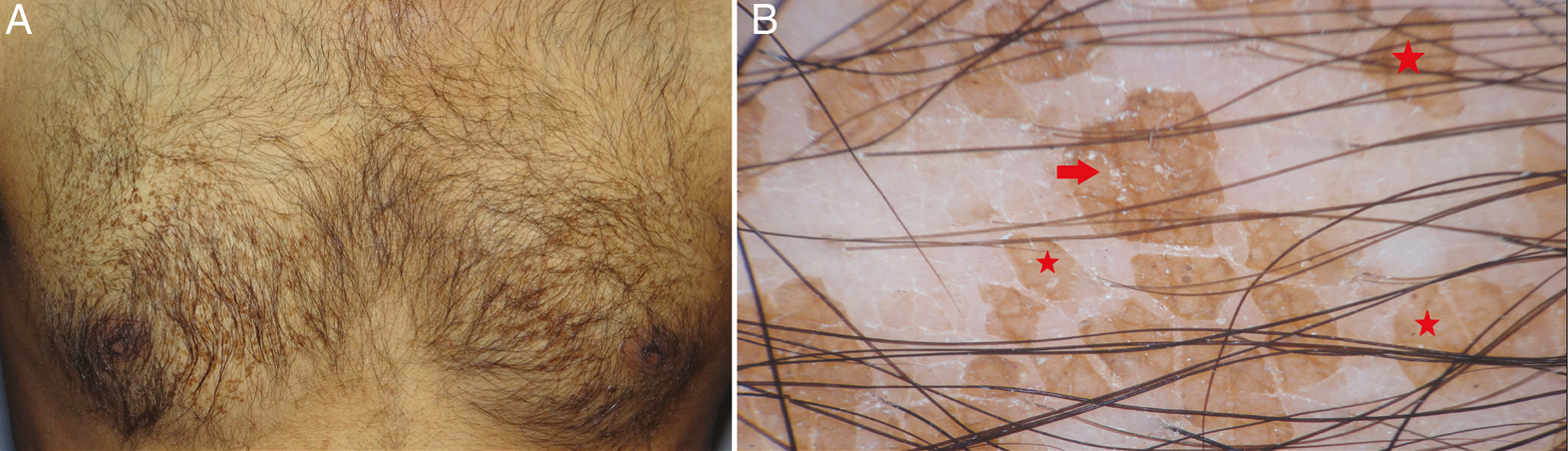
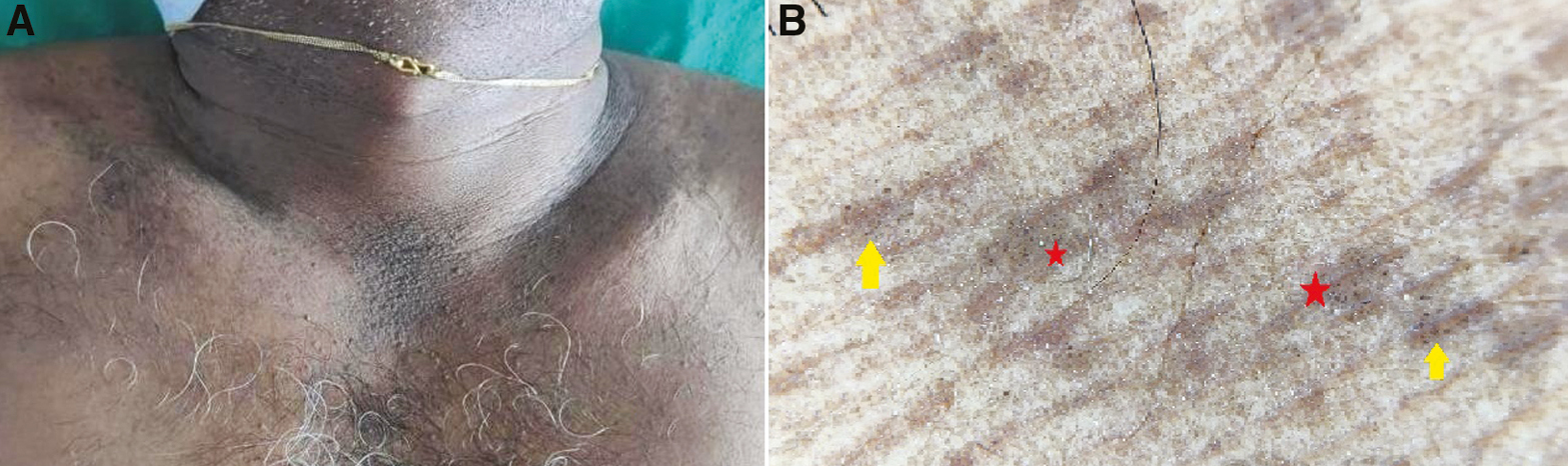
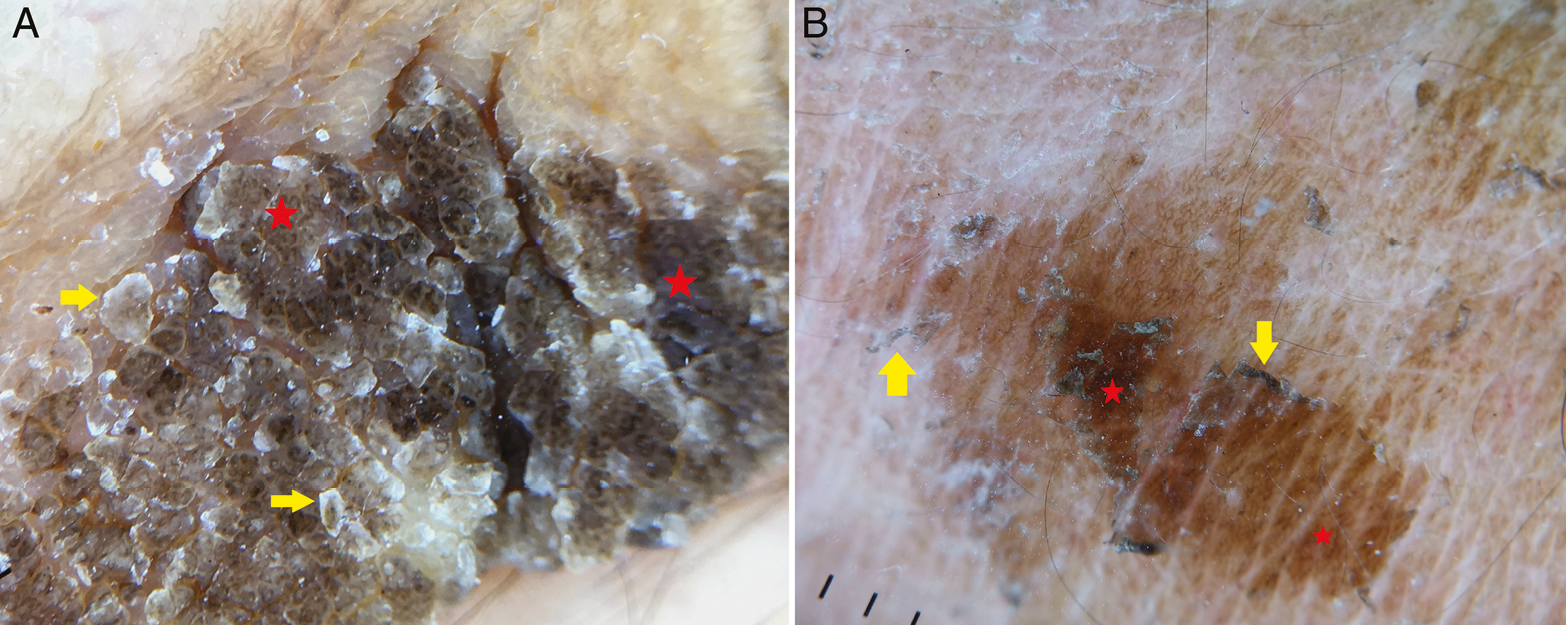
- (A) Clinical image of confluent reticulated papillomatosis with dirty-looking hyperpigmented papules on the neck. (B) Dermoscopy shows ridges (red arrow) and fissures (yellow arrow) and brown globules in a “cobblestone” pattern (yellow circle). Scales in the fissures (black arrow) and white areas (yellow star) are well appreciated (Illuco 1100 IDS, Polarized, 10x)
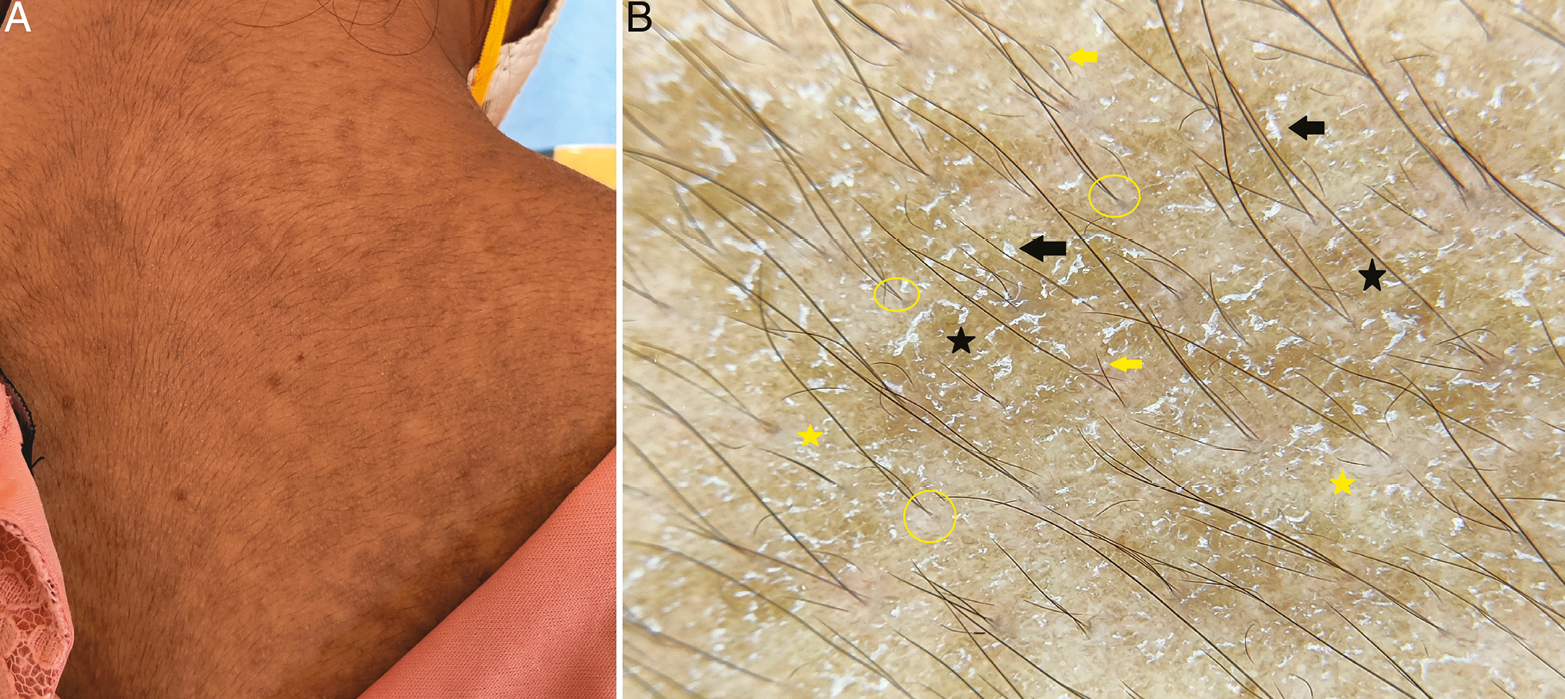
- (A) Clinical image of confluent reticulated papillomatosis with dirty-looking hyperpigmented and hyperkeratotic papules on the back. (B) Dermoscopy shows brown globules (black stars) with surface scales (black arrows) and focal white areas (yellow stars). Note the broken hairs (yellow arrows) and V-like hairs (yellow circles) (Illuco 1100 IDS, Polarized, 10x)
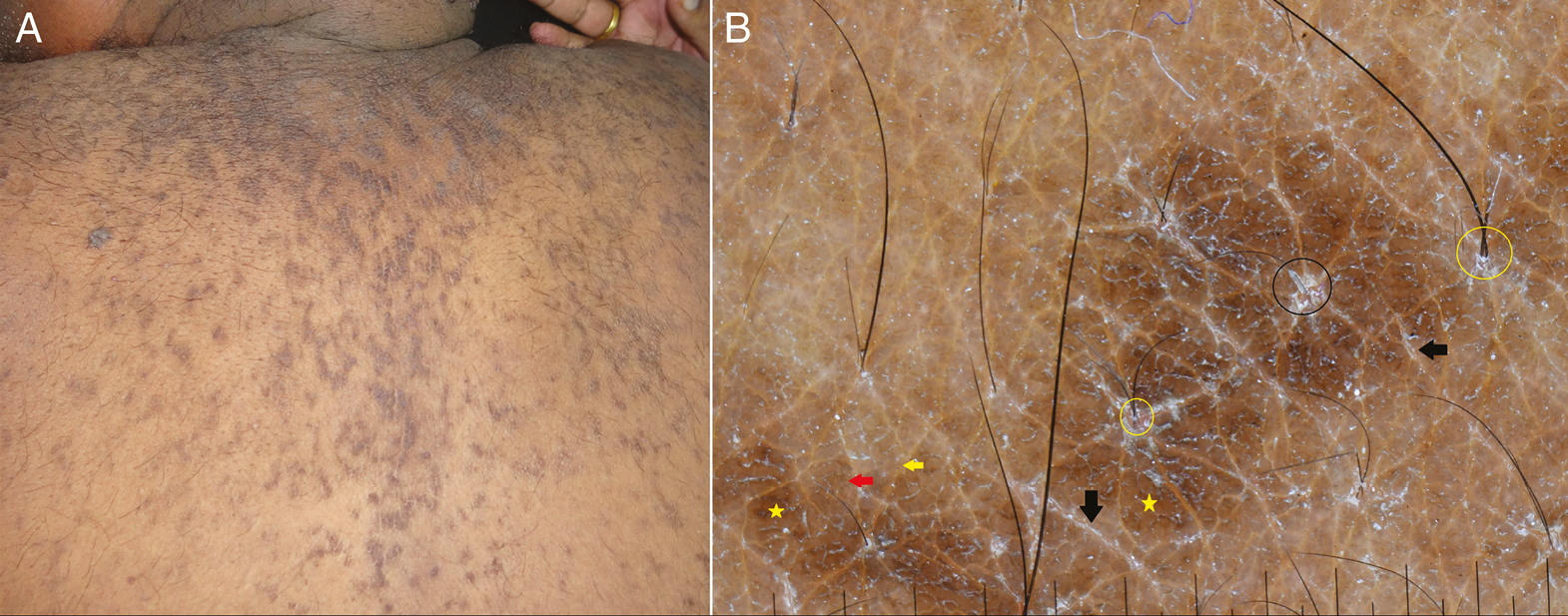
- (A) Clinical image of confluent reticulated papillomatosis showing dirty-looking hyperkeratotic papules in a reticulated pattern on the back. (B) Dermoscopy shows ridges (red arrow) and fissures (yellow arrow) and brown globules in a “cobblestone” pattern (yellow stars). Scales in the fissures (black arrows) and around follicles (black circles) are seen. Note the V-hair (yellow circles) (Illuco 1100 IDS, Polarized, 10x)
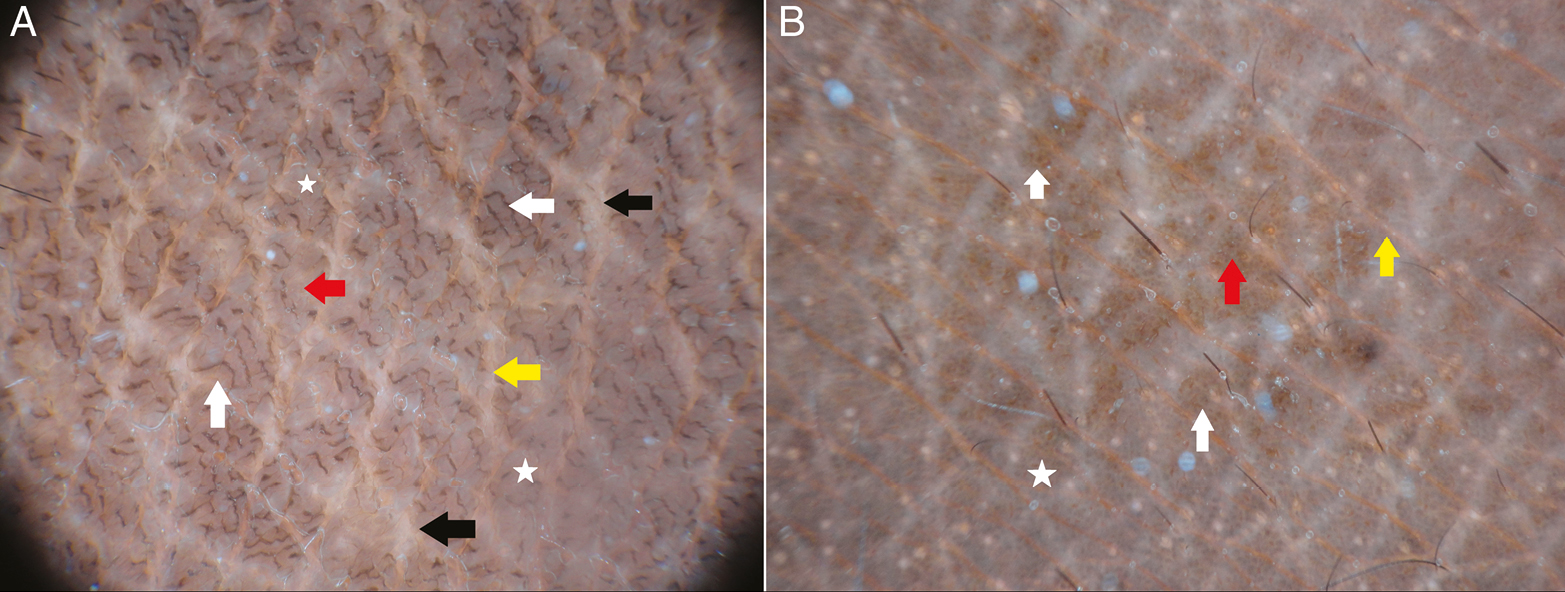
- Dermoscopic image of confluent reticulated papillomatosis (A) and (B) shows ridges (red arrow) and fissures (yellow arrow) in a cerebriform pattern. Note the grayish-brown globules (white stars) and linear brown globular structures (white arrows) with focal white areas (black arrows) (A). Brown (white arrows) and grayish-black globules (white star) are seen (Illuco 1100 IDS, Polarized, 10x)
- (A) Clinical image of terra firma-forme dermatosis showing hyperkeratotic, dirty-looking papules on the chest. (B) Dermoscopy shows polygonal yellowish-brown globules (red stars) with regular margins. Scales are seen on the surface and edge of globules (red arrow). Global view gives an impression of a “mosaic” pattern (Illuco 1100 IDS, Polarized, 10x)
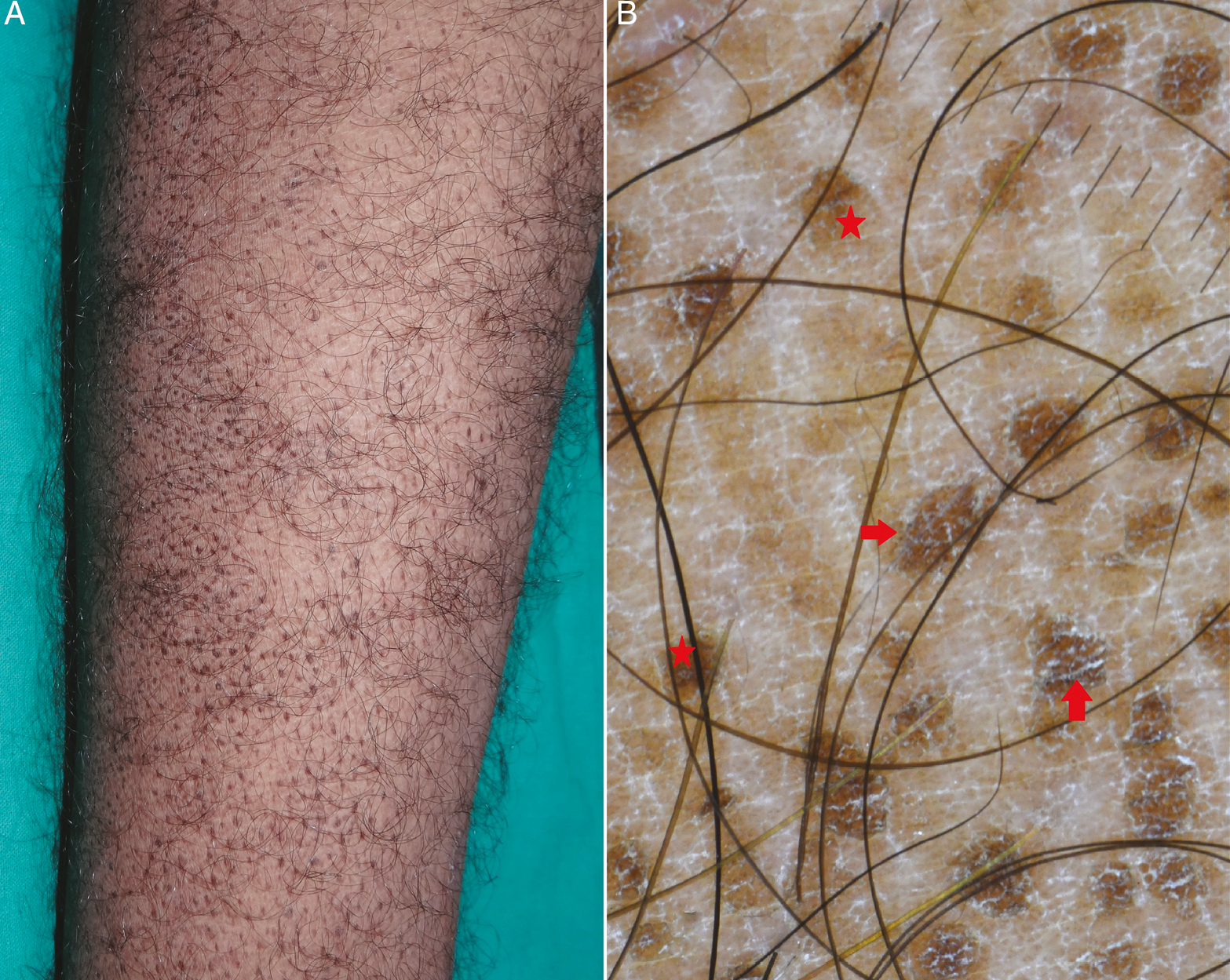
- (A) Clinical image of terra firma-forme dermatosis showing hyperkeratotic, dirty-looking papules on the lower limb. (B) Dermoscopy shows a “mosaic” pattern in global view. Polygonal yellowish-brown globules (red stars) with regular margins are well appreciated. Scales are seen on the surface and edge of globules (red arrow) (Illuco 1100 IDS, Polarized, 10x)
- (A) Clinical image of terra firma-forme dermatosis showing hyperkeratotic, dirty-looking papules on the trunk. Area is marked for alcohol swab test.(B) Dermoscopy shows a “mosaic” pattern in global view. Polygonal yellowish-brown globules (red stars) with regular margins are well appreciated. Scales are seen on the surface and edge of globules (red arrow). Note the black dots (yellow arrows) studded on the pigment globules (Illuco 1100 IDS, Polarized, 10x)
- (A) Clinical image of terra firma-forme dermatosis showing disappearance of papules on alcohol swab test. (B) Dermoscopy shows the absence of yellowish-brown globules. A few scales are noted (red arrows) (Illuco 1100 IDS, Polarized, 10x)
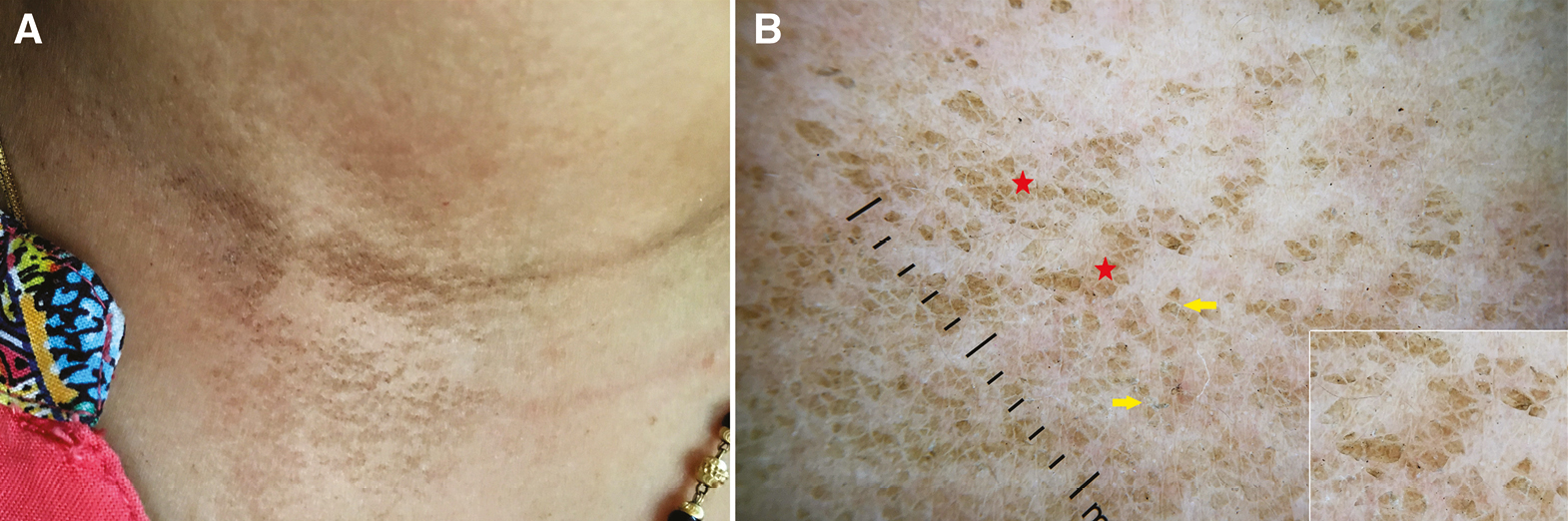
- (A) Clinical image of terra firma-forme dermatosis showing hyperkeratotic, dirty-looking papules on anterior neck. (B) Dermoscopy shows regular arrangement of brown globules (red stars) studded with black dots (yellow arrows) (Illuco 1100 IDS, Polarized, 10x)
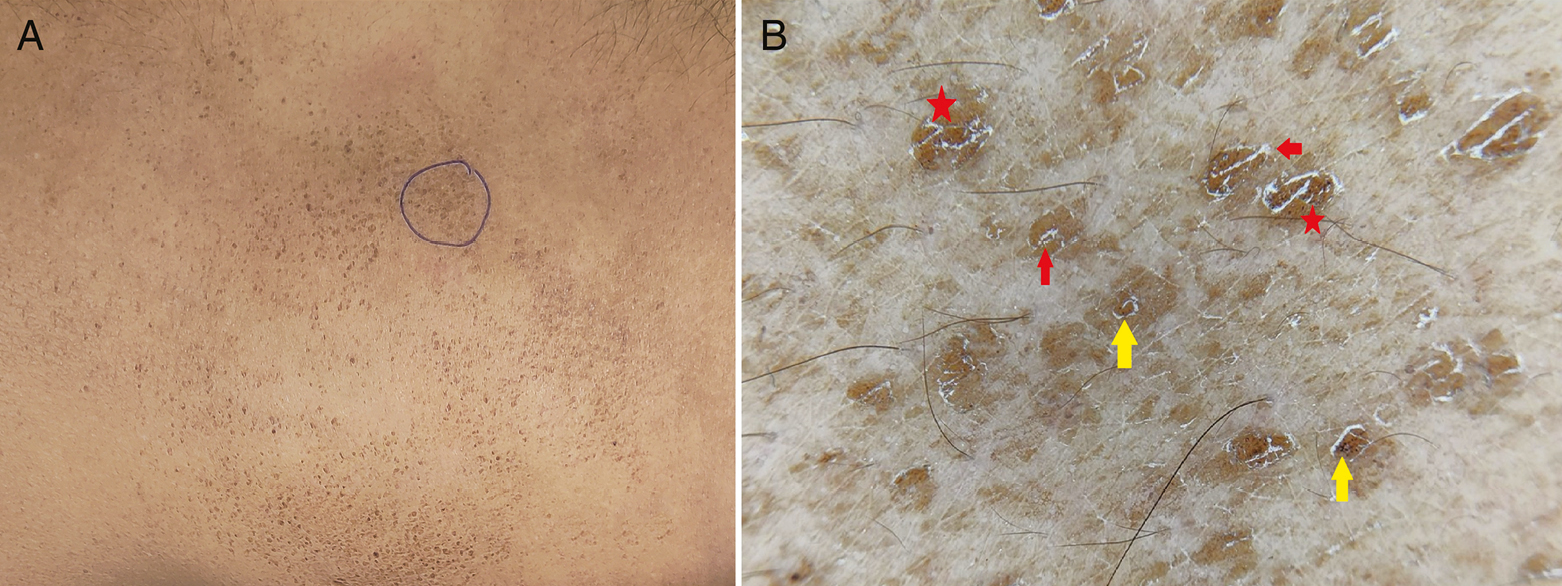
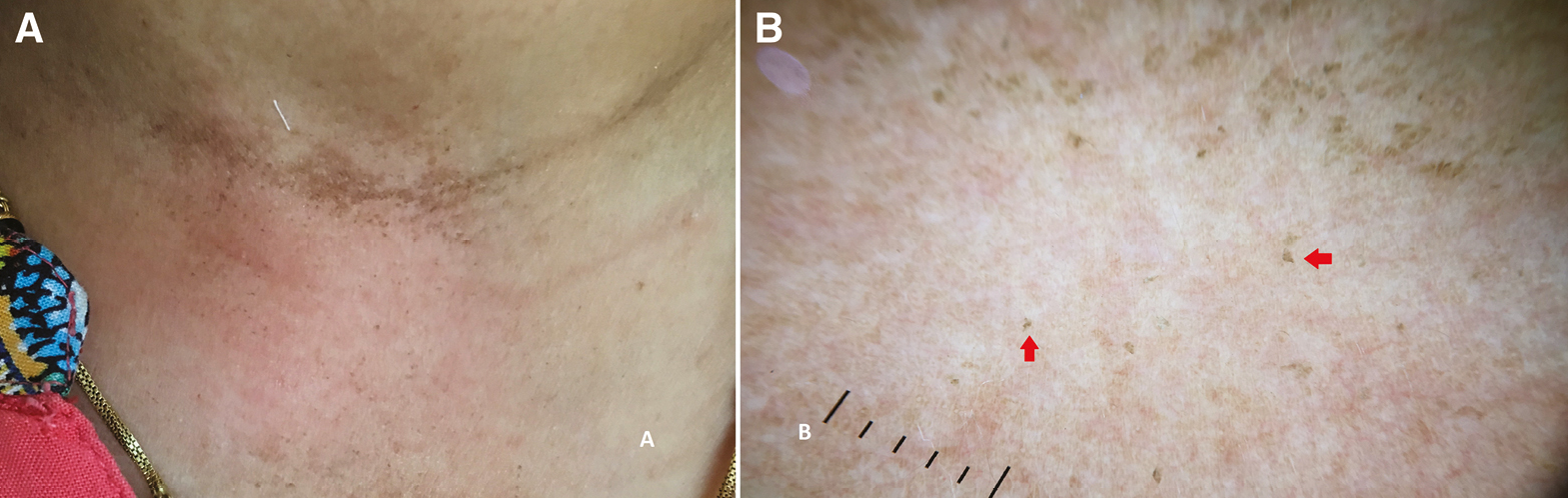
- (A) Clinical image of dermatitis neglecta showing hyperkeratotic and hyperpigmented, dirty-looking papules on anterior neck. (B) Dermoscopy shows irregular brown globules (red stars) with everted edges (yellow arrows), giving a “cornflake-like” appearance. Inset depicts close-up view (Illuco 1100 IDS, Polarized, 10x)
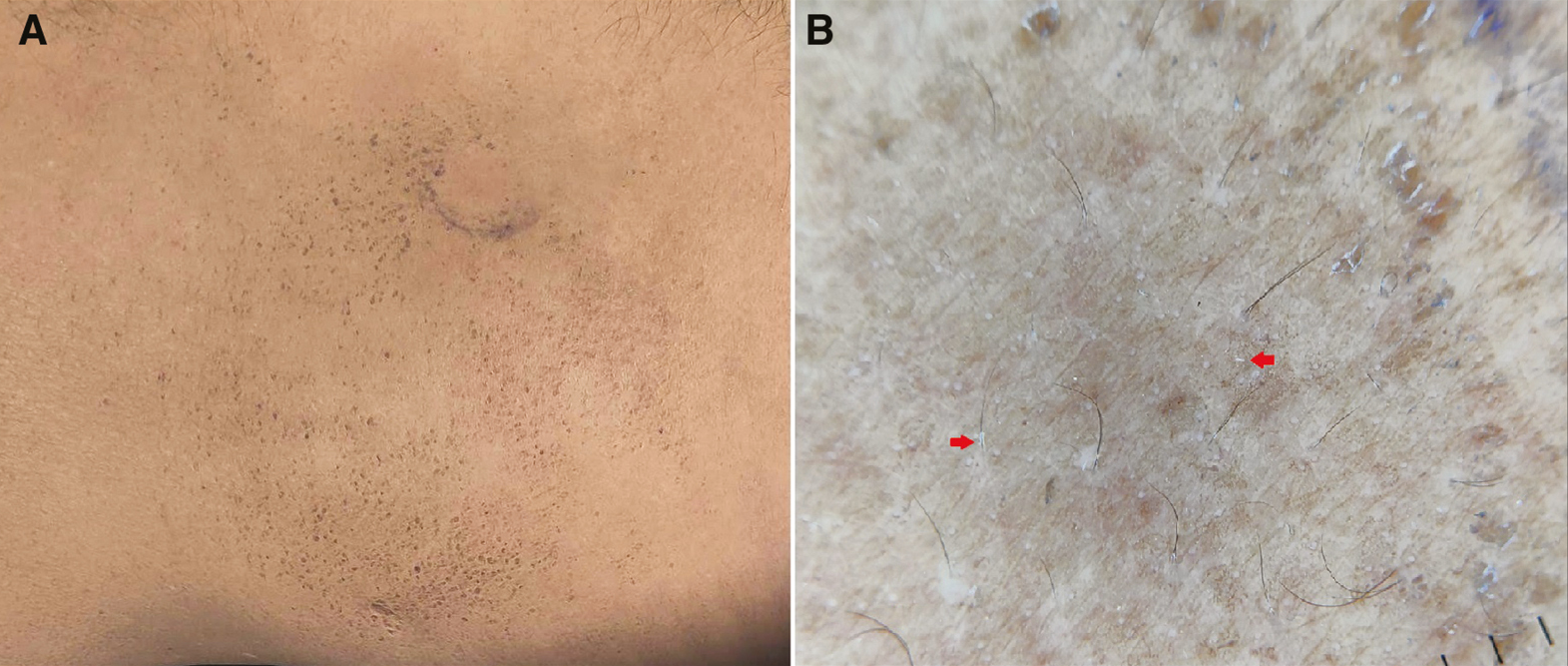
- (A) Clinical image of dermatitis neglecta showing disappearance of papules on soap water swab test. (B) Dermoscopy shows the absence of brown globules. A few scales (red arrows) are noted (Illuco 1100 IDS, Polarized, 10x)
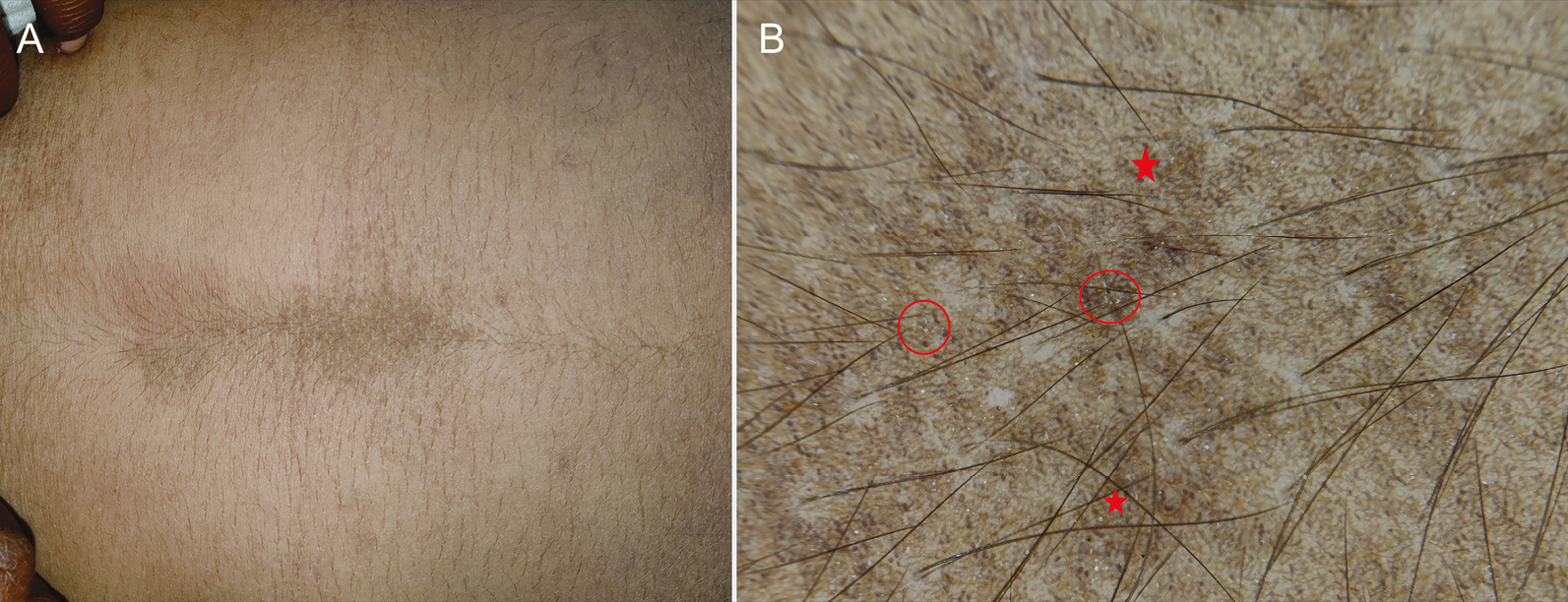
- (A) Clinical image of dermatitis neglecta showing hyperkeratotic and hyperpigmented, dirty-looking papules on the abdomen. (B) Dermoscopy shows an irregular arrangement of blackish-brown globules and dots (red stars) and scales (red circles) (Illuco 1100 IDS, Polarized, 10x)
- Dermoscopic image of dermatitis neglecta (A and B) shows irregular brown globules (red stars) with everted edges (yellow arrows), giving a “cornflake-like” appearance (Illuco 1100 IDS, Polarized, 10x)
| Dermoscopic features | CRP | TFFD | DN |
|---|---|---|---|
| Morphological structures | Brown pigment globules Ridges and fissures Focal white areas |
Polygonal yellowish-brown globules with studded black dots | Irregular blackish-brown or brown globules |
| Follicular changes | Broken hairs V-like hairs |
None | None |
| Scales | Perifollicular In the fissures |
On the surface and at the periphery of the globules | On the surface and at the periphery of the globules |
| Definitive pattern of pigment globules | “Cobblestone” pattern | “Mosaic” pattern | “Cornflake-like” pattern |
| Dermoscopic variables | CRP (n = 30) | TFFD (n = 20) | DN (n = 12) | P Value* |
|---|---|---|---|---|
| Scales | 30 (100%) | 15 (75%) | 6(50%) | 0.003 |
| Follicular changes | 25 (83.33%) | – | – | – |
| White areas | 30 (100%) | – | – | – |
| Black dots | – | 5 (25.00%) | – | – |
| Pigmentation of globules/dots | ||||
| 1. Brown | 28 (93.33%) | 2 (10.0%) | 6(50%) | 0.001 |
| 2. Yellow | – | 16 (80%) | 2(16.66%) | 0.004 |
| 3. Black | 2 (6.66%) | 2 (10.0%) | 4 (33.33%) | 0.06 |
*Chi-square test
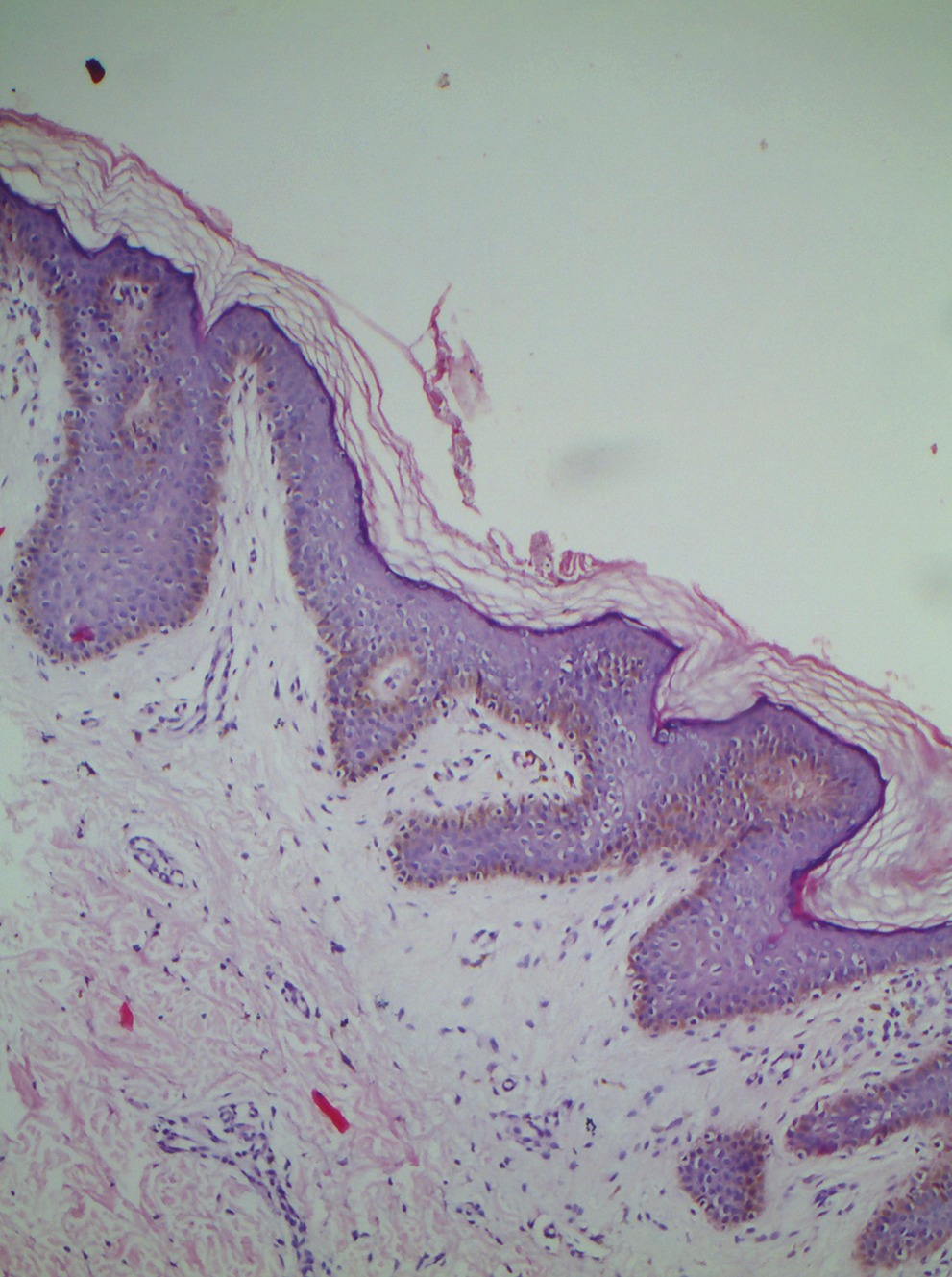
- Histopathology of confluent reticulated papillomatosis showing basket-weave hyperkeratosis, focal acanthosis, increased melanin in basal layer hyperpigmentation, and papillomatosis (H and E, 10x)
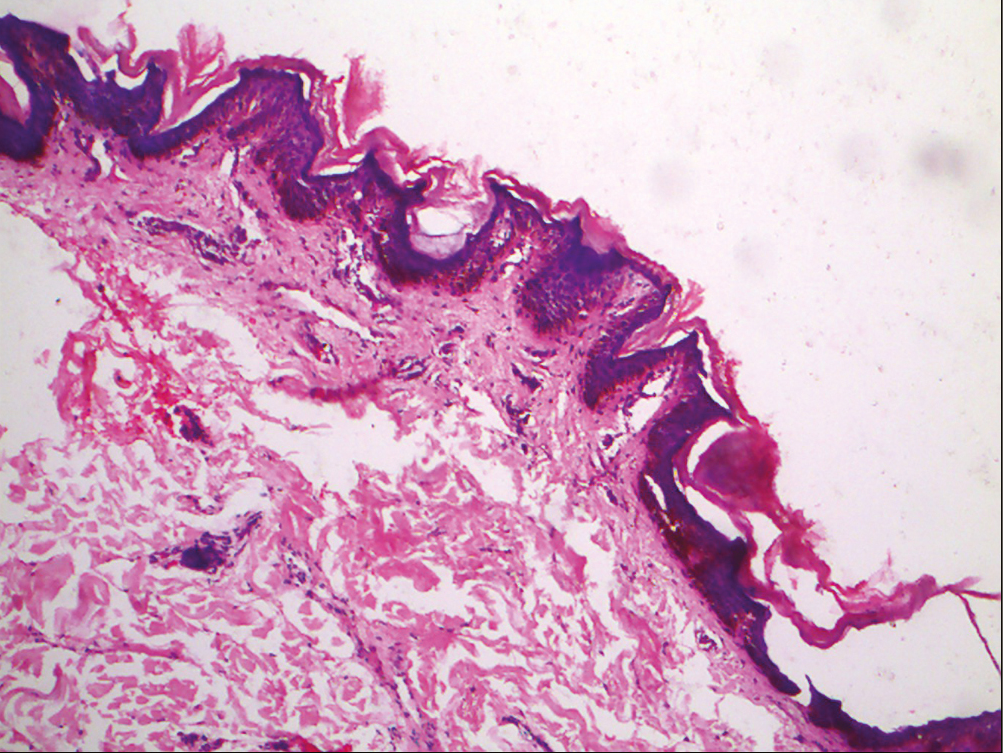
- Histopathology of terra firma-forme dermatosis showing lamellar hyperkeratosis and papillomatosis with melanin deposition within the basal layer (H and E, 10x)
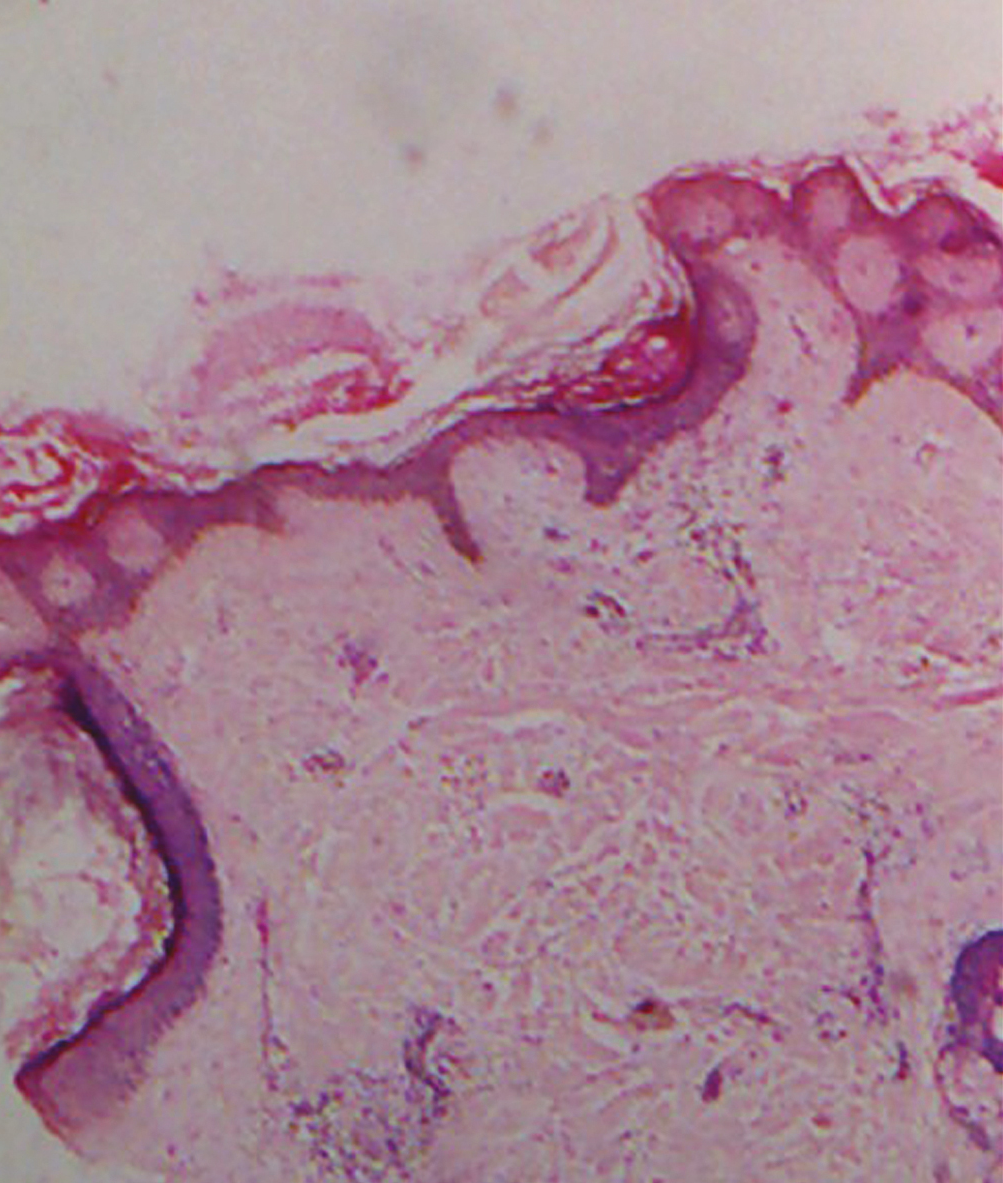
- Histopathology of dermatitis neglecta showing compact ortho-hyperkeratosis, papillomatosis, and increased melanin in the epidermis (H and E, 10x)
DISCUSSION
The CRP is an uncommon dermatological condition with abnormal keratinization, which was believed to be due to an exaggerated response to Malassezia spp. Later, Dietzia papillomatosis was confirmed to be implicated in the development of CRP.[7] It typically presents as multiple brown to black hyperpigmented papules that coalesce in the center and demonstrate reticulation toward the periphery. It involves the neck, anterior chest and abdomen, infra-scapular, and sub-mammary areas. It is usually asymptomatic, although occasional pruritus may be present.[2]
In this study, dermoscopy of CRP showed a ridges and fissures (gyri and sulci) pattern resembling a cerebriform pattern. Brown globules were situated on the ridges and were separated by white striae or lines, giving a characteristic “cobblestone” appearance. Focal white areas were noted in between the ridges and fissures. The ridges were brownish and fissures were whitish, resulting in alternating white and brown colors on the background. The mentioned dermoscopic patterns were in line with previous reports.[58] Interestingly, follicular changes such as broken hairs, V-hair were observed particularly on the fissures. This observation substantiates the previous observation of hair changes in CRP.[91011] Scales were located in perifollicular areas and along skin furrows. However, scales can also be in a diffuse pattern.[8] Thus, dermoscopy displays distinctive features in CRP.
TFFD is a benign and acquired condition that presents with dirt-like plaques. The literal meaning of “terra firma” is “solid land” in Latin language. It is also known as Duncan’s dirty dermatosis.[12] Clinical features include asymptomatic dirty-looking black or brown plaques that are distributed mainly on the neck, face, trunk, and ankles. The lesions are classically resistant to soap water swabbing but can be removed by rubbing with 70% ethyl alcohol, which acts as both a diagnostic and a therapeutic tool.[12] Dermoscopy revealed characteristic polygonal plate-like yellowish-brown globules. The global view resembled a “mosaic” pattern. Scales were noted on the surface and periphery of the globules. Similar dermoscopic features were described in previous literature.[1113] On the other hand, black dots, which were studded on the pigment globules, were found [Figures 7 and 9]. This was a new observation in this study. This is probably due to heavy melanin in the skin of color. Second, pigmentation was yellowish-brown rather than brown. This disparity could be explained on the basis of excessive serum entrapped in the hyperkeratotic lesions. Hence, dermoscopy demonstrates a definitive pattern in TFFD.
DN, popularly known as unwashed dermatitis, is an uncommon dermatosis. Predisposing factors such as immobility due to surgery or paralysis, pain, hyperesthesia, and local trauma result in improper cleaning and inadequate exfoliation. The excessively retained and accumulated sebum, dirt, keratin, and sweat give localized hyperpigmented papules and plaques, which appear as dirty-looking lesions. The lesions can be easily removed by vigorous rubbing with soap water or alcohol swabs.[14] In the present study, dermoscopy demonstrated irregular blackish-brown globules with everted edges, giving a classical appearance of a “cornflake-like” pattern. Scales, similar to TFFD, were found on the surface and periphery of the globules. Dermoscopic patterns were in accordance with published reports.[1315] Therefore, dermoscopy showed patterns that were definitive in CRP, TFFD, and DN.
The histopathology of CRP shows basket-weave hyperkeratosis, focal acanthosis limited to areas of elongation of rete ridges, basal layer hyperpigmentation, and papillomatosis.[9] The ridges and fissures correspond to papillomatosis, and scales are due to hyperkeratosis. Brown globules correlate with intense pigment in the epidermis. White areas represent basket-weave hyperkeratosis in epidermis in the adjacent valley [Figure 17].
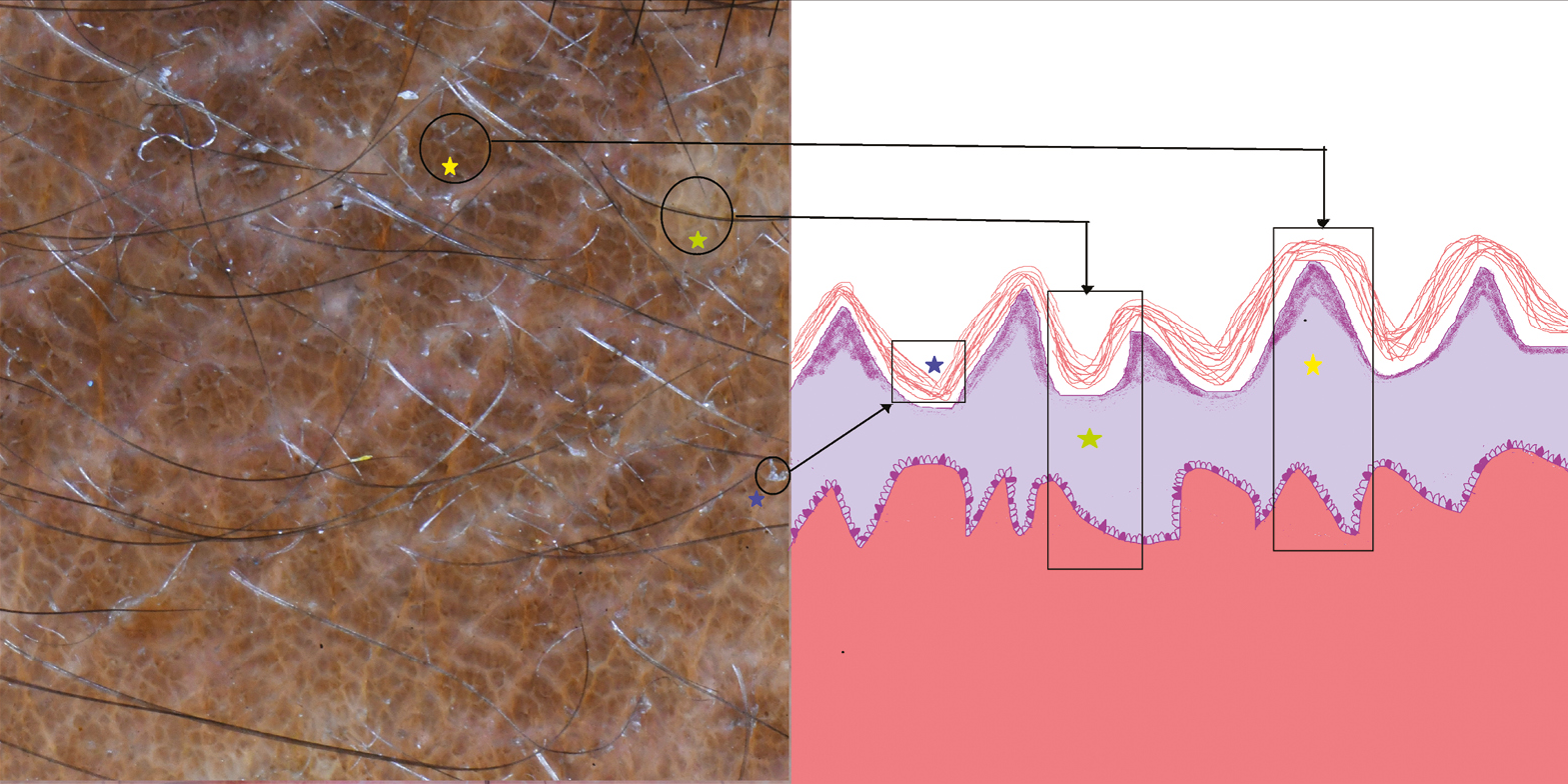
- Schematic of confluent reticulated papillomatosis showing dermoscopic and histopathological correlation, ridge with papillomatosis (yellow stars), white areas with hyperkeratosis, and atrophic epidermis in the valley (green stars) and scales with hyperkeratosis (blue stars)
The histopathology of TFFD reveals lamellar hyperkeratosis with compact orthokeratosis and papillomatosis. Melanin deposition was noted within the basal layer and in the hyperkeratotic areas as well.[16] Polygonal plate-like yellowish-brown globules represent papillomatosis and acanthosis. Black dots correspond to melanin in the epidermis [Figure 18].
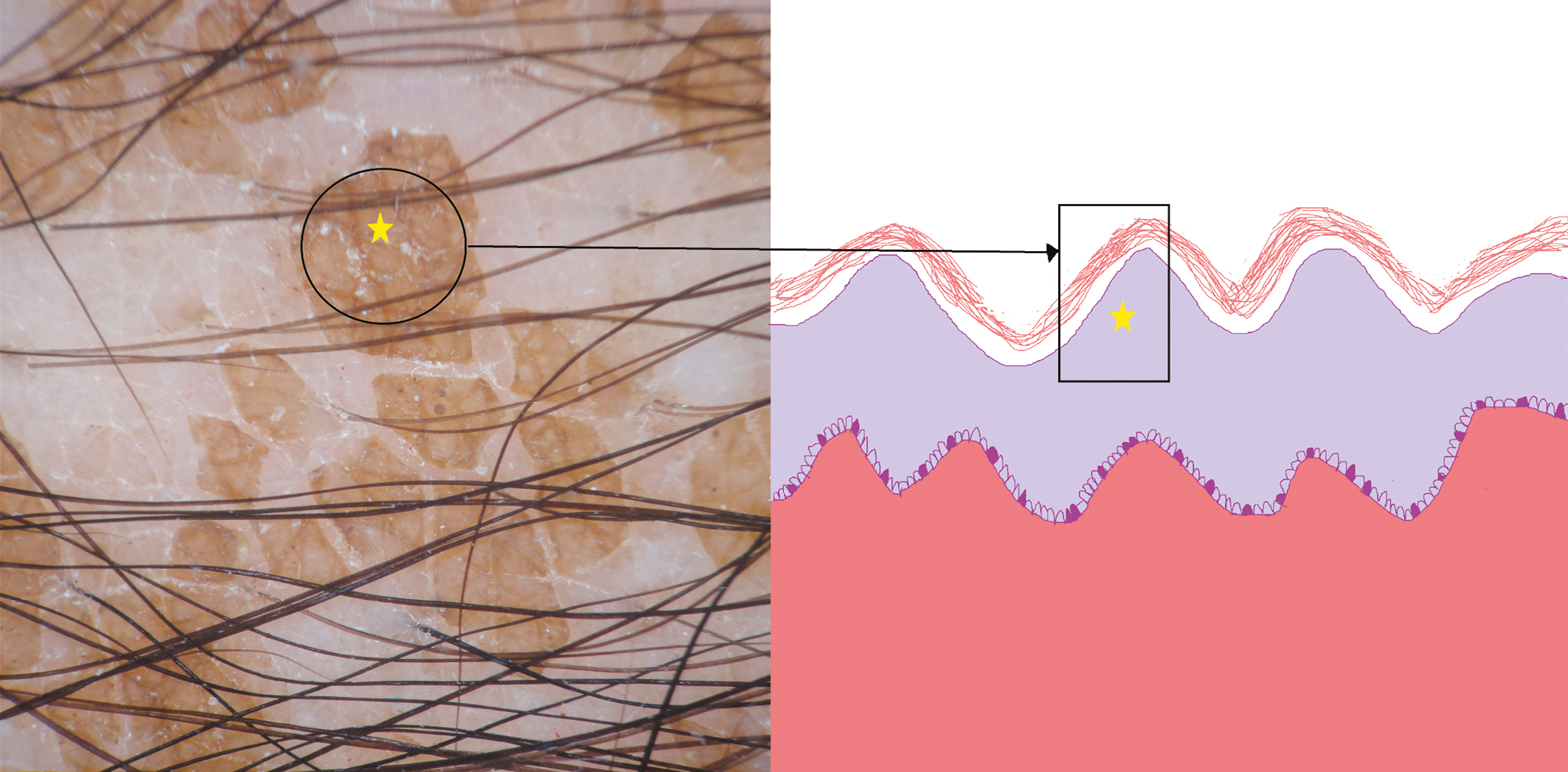
- Schematic of terra firma-forme dermatosis showing dermoscopic and histopathological correlation; yellowish-brown globules with papillomatosis and acanthosis (yellow stars)
Histopathology of DN reveals compact ortho-hyperkeratosis, papillomatosis, and acanthosis with absent or sparse inflammation.[17] Scales are due to hyperkeratosis and blackish-brown globules result from the stacking of stratum corneum, debris, and dirt [Figure 19]. Thus, dermoscopic features in CRP, TFFD, and DN were well correlated with corresponding histopathological changes.
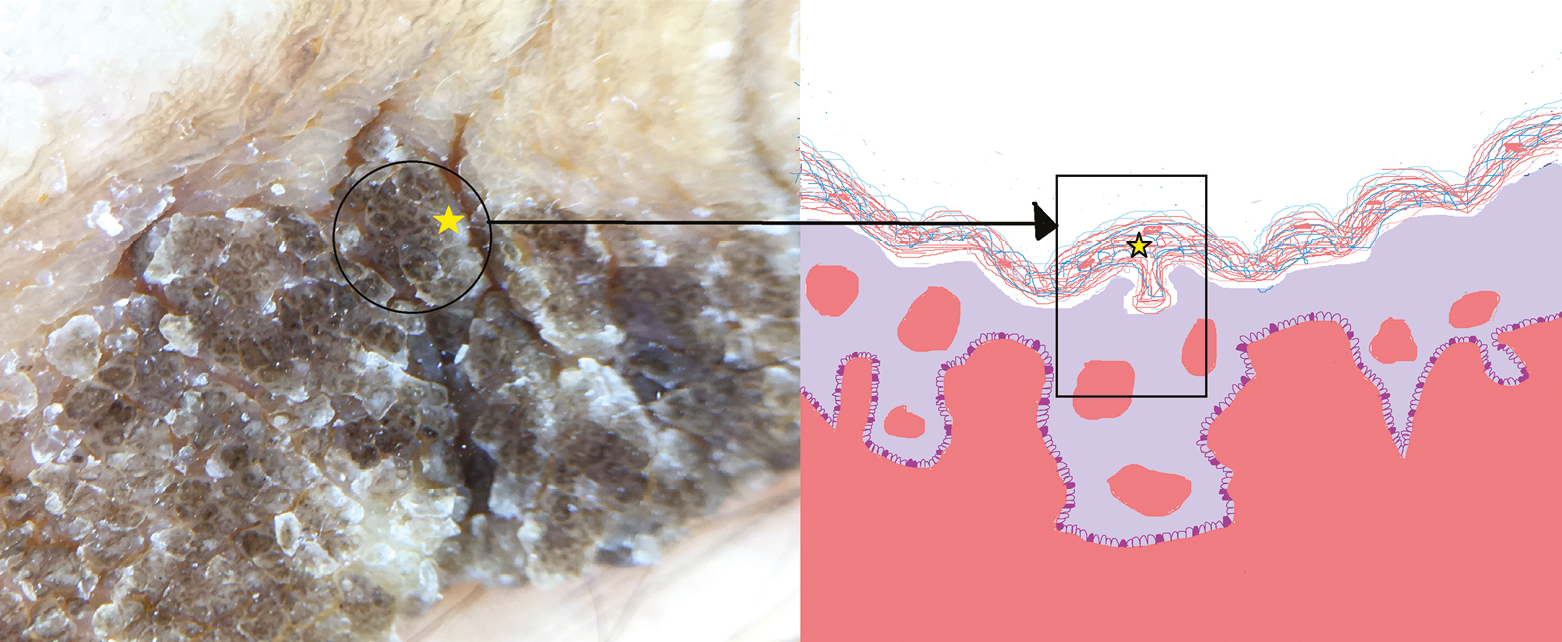
- Schematic of dermatitis neglecta showing dermoscopic and histopathological correlation; blackish-brown globules with stacking of stratum corneum, debris, and dirt (yellow stars)
It should be noted that TFFD and DN are distinguishable by a bedside test, such as swab tests. Nevertheless, dermoscopy is rapid, and it demonstrates characteristic and discernible patterns in both conditions. The data are documented by a dermoscopic examination, which can act as an evidence-based practice of dermatology. Although histopathology is the gold standard in the confirmation of diagnosis in CRP, dermoscopy shows definitive patterns, which are evident by reports in the literature and in this study as well.
In a nutshell, pigment globules were present in all three conditions but with subtle differences in color, morphology, and arrangement. In CRP, brown pigment globules were in a “cobblestone” pattern; in TFFD, polygonal plate-like yellowish-brown globules were in a “mosaic” pattern. Inversely, blackish-brown globules with everted edges (cornflake-like) were distributed irregularly in DN. There was a statistically significant difference in the color of pigment in each condition, with p values of –0.001 and 0.004. In addition, CRP was typified by focal white areas, fissures and ridges, and hair changes. These changes were not observed in TFFD and DN. Scales in dermoscopy have a potential value in the proper diagnosis of many conditions.[18] Their morphology and arrangement gives a clue. Collarette scales are found in pityriasis rosea, whereas scales are bright white in psoriasis.[19] In the present study too, the morphology of scales was consistently distinctive, being perifollicular in CRP, and at the periphery and on the surface of pigment globules in both TFFD and DN. This observation was statistically highly significant with a p value of –0.003.
CONCLUSION
CRP, TFFD, and DN manifest with hyperkeratotic, hyperpigmented, and dirty-looking papules and plaques. Dermoscopy is a rapid and an in vivo diagnostic method in the diagnosis and in the differentiation of CRP, TFFD, and DN. It comes in handy in the accurate and evidence-based diagnosis of these conditions. It acts as an adjunctive diagnostic method in the daily practice of clinical dermatology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Hyperpigmented disorders (disorders of pigmentation) In: Lallas A, Errichetti E, Ioannides D, eds. Dermoscopy in general dermatology. London: CRC Press; 2019. p. :257-69.
- [Google Scholar]
- Confluent and reticulate papillomatosis: A retrospective study from southern India. Indian Dermatol Online J. 2021;12:90-6.
- [Google Scholar]
- Bilaterally symmetrical terra firma-forme dermatosis: A diagnostic conundrum. Egypt J Dermatol Venerol. 2018;38:46-8.
- [Google Scholar]
- Dermatosis neglecta in a case of multiple fractures, shoulder dislocation and radial nerve palsy in a 35-year-old man: A case report. J Med Case Rep. 2008;2:347.
- [Google Scholar]
- Dermoscopy in general dermatology: A practical overview. Dermatol Ther (Heidelb). 2016;6:471-507.
- [Google Scholar]
- Confluent and reticulated papillomatosis: Diagnostic and treatment challenges. Clin Cosmet Investig Dermatol. 2016;9:217-23.
- [Google Scholar]
- Confluent and reticulate papillomatosis of gougerot-carteaud and obesity: Dermoscopic findings. An Bras Dermatol. 2014;89:507-9.
- [Google Scholar]
- Dermoscopic patterns in confluent and reticulated papillomatosis: A case report. Our Dermatol Online. 2016;7:323-26.
- [Google Scholar]
- Dermoscopic approach to hyperpigmented lesions in skin of color. Clin Dermatol Rev. 2020;4:84-91.
- [Google Scholar]
- Dermatoscopic features of pigmentary diseases in ethnic skin. Indian Dermatol Online J. 2021;12:24-33.
- [Google Scholar]
- Terra firma-forme dermatosis: A report of ten individuals with Duncan’s dirty dermatosis and literature review. Dermatol Pract Concept. 2015;5:29-33.
- [Google Scholar]
- Dermoscopy in terra firma-forme dermatosis and dermatosis neglecta. Int J Dermatol. 2017;56:1481-3.
- [Google Scholar]
- Terra firma-forme dermatosis: An underdiagnosed condition. An Bras Dermatol. 2020;95:397-9.
- [Google Scholar]
- Dermatitis neglecta – a dirty dermatosis: Report of three cases. Indian J Dermatol. 2015;60:185-7.
- [Google Scholar]
- Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the international dermoscopy society. Br J Dermatol. 2020;182:454-67.
- [Google Scholar]
- Accuracy of dermoscopic criteria for the diagnosis of psoriasis, dermatitis, lichen planus and pityriasis rosea. Br J Dermatol. 2012;166:1198-205.
- [Google Scholar]




