
Translate this page into:
Eccrine Syringofibroadenoma: A Rare Skin Adnexal Tumor at a Rare Site
Address for correspondence: Dr. Aditya Kumar Bubna, Department of Dermatology, Katihar Medical College, Karim Bagh, Katihar 854106 Bihar, India. E-mail: zimbabwa21@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
Eccrine syringofibroadenomas (ESFAs) are rare benign skin adnexal tumors (SATs) that arise from cells of the acrosyringium of eccrine sweat glands.[1] Clinically, varied phenotypes have been reported but histological findings of ESFA are classical, enabling the dermatologist to arrive at a conclusive diagnosis.
The three characteristic findings identified on histopathology in ESFA include:
Narrow strands of basaloid acrosyringeal cells arranged as anastomosing cords extending into the dermis.
Duct formation.
Mucinous fibrovascular stroma.
Our patient was a 25-year-old male, who presented with an asymptomatic, pinkish white fibrotic nodule over the scalp of size 2 × 2.5 cm [Figure 1]. He noticed this since the past 7 months and the lesion had gradually progressed to attain the current status. A provisional diagnosis of fibroma and SAT were considered and an excision biopsy was performed. Skin biopsy revealed thin anastomosing cords of epithelial cells arising from the epidermis and extending toward the dermis [Figures 2 and 3].

- A solitary pinkish white fibrotic nodule on the scalp
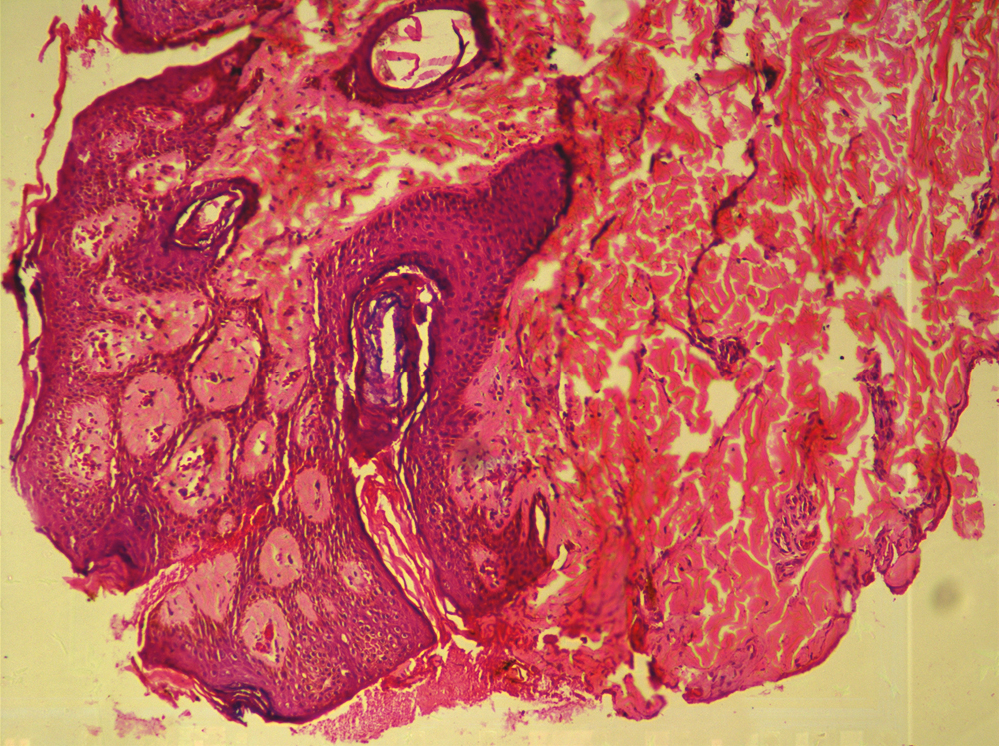
- Thin anastomosing cords of epithelial cells arising from the epidermis and extending to the dermis (H&E ×40)
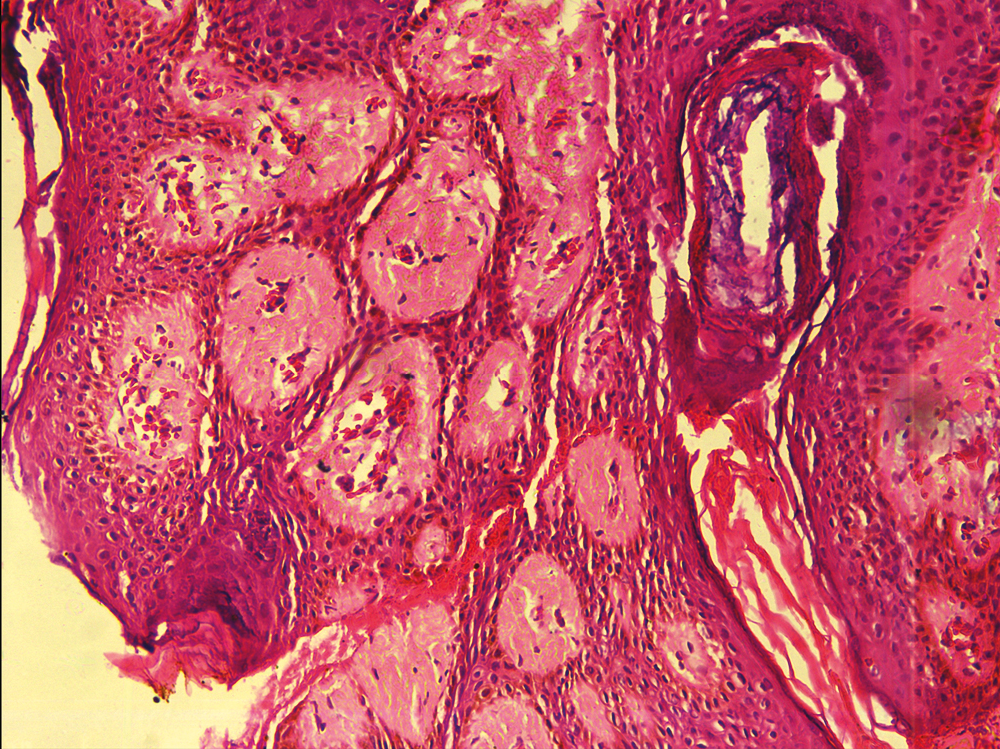
- Higher magnification of anastomosing cords composed of epithelial cells (H&E ×100)
A ductule lined by cuboidal cells was also identified in association with the epithelial strands suggesting eccrine differentiation [Figure 4]. With the aforementioned findings, a diagnosis ESFA was confirmed.
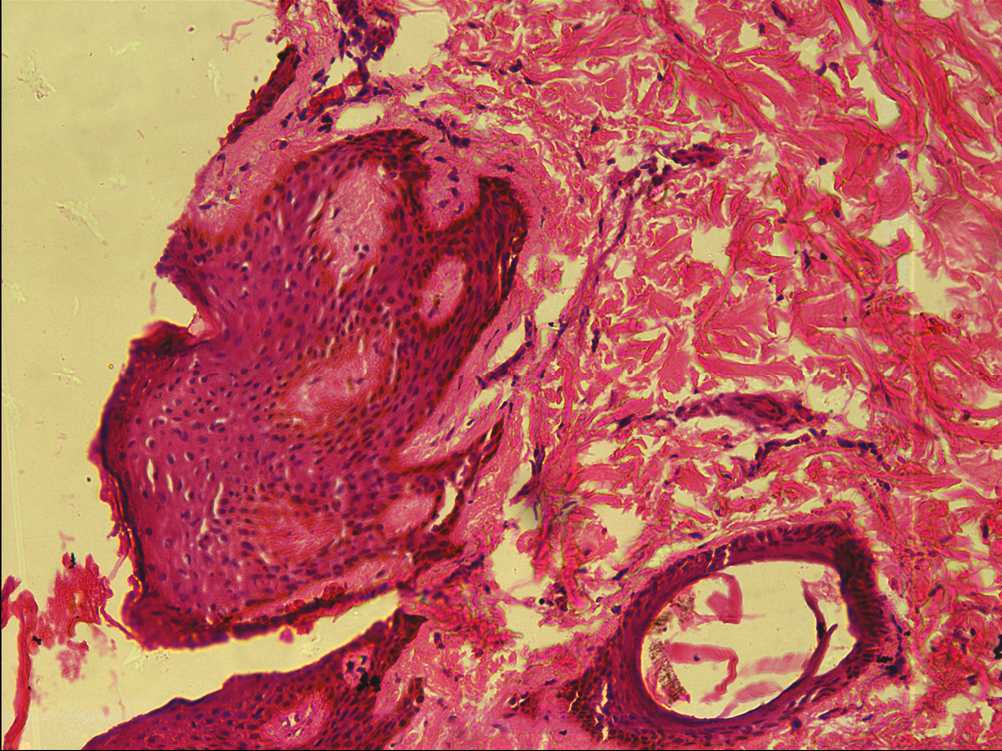
- A ductule lined by cubical cells in association with epithelial strands, suggesting eccrine differentiation (H&E ×100)
Five clinical subtypes of ESFA exist; namely:
Solitary ESFA;
Multiple ESFA associated with ectodermal dysplasia;
Multiple ESFA without cutaneous features;
Unilateral linear ESFA; and
Reactive ESFA associated with inflammatory or neoplastic dermatosis.
Our patient belonged to the solitary ESFA subtype. Past medical literature elaborates very few reports on solitary non-reactive ESFAs; details of which have been outlined in Table 1.
| Serial number | Author(s) | Year | Age/sex | Duration | Symptoms | Location | Morphology |
|---|---|---|---|---|---|---|---|
| 1. | Bottino et al.[2] | 2015 | 81 years/female | 3 years | Painful | Right lateral malleoli | Erythematous tumor-like plaque with small central ulceration |
| 2. | Arora et al.[3] | 2015 | 62 years/male | 1 year | Painful | Distal phalanx of left index finger | Sharply demarcated nodular plaque with thick, adherent scales and a warty, keratotic surface |
| 3. | Hurt et al.[4] | 1990 | 48 years/male | 1 year | Asymptomatic | Right lumbar region | A solitary 10 × 7 mm papule |
| 4. | Kanitakis et al.[5] | 1987 | 80 years/male | — | — | Right great toe | Solitary nodule resembling granuloma pyogenicum |
| 5. | Mehregan et al.[6] | 1985 | 72 years/male | 15 years | — | Left wrist | 5 × 2.5 cm solitary, verrucous, and nodular growth partially covered by a layer of crust |
| 6. | Olmos[7] | 1980 | 67 years/female | — | — | Right hypochondrium | Solitary nodule |
| 7. | Civatte et al.[8] | 1981 | 60 years/male | — | — | Right leg | Solitary nodule |
| 8. | Iqbal et al.[9] | 2019 | 42 years/male | — | Painful | Scalp | Erythematous tender swelling 2.5 × 2 cm resembling a dermoid cyst |
| 9. | Our patient | 2021 | 25 years/male | 7 months | Asymptomatic | Scalp | Pinkish white fibrotic nodule |
After studying the above reports (pertaining to solitary ESFA), we observed that the extremities constituted the most common site of involvement. Scalp involvement, on the other hand was described in only one previous publication.[9] We would hereby like to highlight our case firstly, owing to the rare fibrotic nodular morphology encountered and secondly its involvement of the scalp (an uncommon site for ESFA).
Histopathology findings reported in our patient were classical for this entity and that enabled clinching the diagnosis. Immunohistochemistry, though not mandatory with this classical histopathology may be required for diagnosis in some less typical presentations to confirm eccrine origin of the SAT.
To conclude, all dermatologists should be familiar with the histopathological pattern of ESFA, so that the diagnosis of ESFA is not missed. The standard treatment for solitary ESFA is surgical excision.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Solitary eccrine syringofibroadenoma with nail involvement: A rare entity. Indian J Dermatol. 2015;60:103.
- [Google Scholar]
- Eccrine syringofibroadenoma (Mascaró). An acrosyringeal hamartoma. Arch Dermatol. 1990;126:945-9.
- [Google Scholar]
- Eccrine syringofibroadenoma. Immunohistological study of a new case. Am J Dermatopathol. 1987;9:37-40.
- [Google Scholar]
- Eccrine syringofibroadenoma (Mascaro). Report of two cases. J Am Acad Dermatol. 1985;13:433-6.
- [Google Scholar]
- [Mascaró’s eccrine syringofibroadenoma. Discussion of a case] Med Cutan Ibero Lat Am. 1981;9:193-6.
- [Google Scholar]
- Syringofibroadenoma: Benign eccrine sweat gland tumor—A rare case report. Indian J Dermatopathol Diagn Dermatol. 2019;6:97-9.
- [Google Scholar]




