
Translate this page into:
Efficacy of Intralesional Aqueous Bleomycin in Treatment of Pediatric Lymphatic Malformations
Address for correspondence: Dr. Suhasini Gazula, Department of Pediatric Surgery, Employees State Insurance Corporation (ESIC) Medical College and Superspeciality Hospital, Sanathnagar, Hyderabad, Telangana, India. E-mail: drgazula9@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Introduction:
Lymphatic malformations (LMs) are an aberrant developmental anomaly of dysplastic sequestrated lymphatic vessels. Though surgical excision has been the conventional treatment modality, it has been associated with injury to adjacent structures, recurrences, and poor cosmesis. Intralesional bleomycin has shown a promising role in the treatment of LMs, and we present our experience with aqueous intralesional bleomycin in the pediatric population including infants in terms of its efficacy, complications, and parental satisfaction.
Materials and Methods:
Children with clinically and ultrasound-proven macrocystic non-visceral LMs received aqueous bleomycin intralesionally under ultrasound guidance at 0.5 IU/kg/dose at monthly intervals and not exceeding five doses. Response to therapy and complications were monitored and regression graded as excellent (total disappearance), good (>50% reduction), and poor (<50% reduction).
Results:
Our study included 26 children with a median age of 24 months (range 2–168) and a median weight of 12 kg (range 4–38). The most common site was the neck (37%). Duration of follow-up was 6 years (range 1–7). Response was excellent in 23/26 (88.4%) patients, good in 3/26 (11.5%), and poor in none (0%). Nine (34.6%) patients showed complete response with a single injection. None (0%) developed recurrence. Three (11.5%) children had minor complications such as fever and mild hypopigmentation. None developed any major complications. Parental satisfaction was excellent in 24/26 (92.3%) and good in 2/26 (7.7%) patients.
Conclusion:
Intralesional aqueous bleomycin sclerotherapy is a safe non-surgical intervention for macrocystic pediatric LMs with reasonably good outcomes and even better parental satisfaction.
Keywords
Bleomycin
intralesional
lymphatic malformations
pediatric

INTRODUCTION
Lymphatic malformations (LMs) are an aberrant developmental anomaly of dysplastic sequestrated lymphatic vessels during early embryogenesis, which are lined by endothelial cells with a lymphatic phenotype.[1] LMs most commonly occur in the cervical region but can be found in any organ or system except for the central nervous system. The lesion can be single or multiple and is usually diagnosed in infants before the age of 2 years.[23]
Although surgical excision was the traditional modality of treatment, it is associated with major disadvantages such as risk of injury to vital structures, difficulty in achieving total resection with discrete margins resulting in recurrences, and unappealing cosmesis [Figure 1]. Hence, alternative options were sought after, and injection sclerotherapy with various agents was described.[4] Intralesional bleomycin, an anti-cancer drug, was used as a sclerosing solution for the first time by Yura et al.[5] in 1977. We present our institutional experience with the use of aqueous bleomycin as an intralesional sclerosing agent in pediatric LMs and endorse its use as first-line treatment for non-visceral macrocystic LMs in children.

- Surgical excision of a forearm lymphatic malformation in a child resulting in recurrence and poor cosmesis
MATERIALS AND METHODS
The study was approved by the Institutional Ethics Committee, Employees State Insurance Corporation (ESIC) Medical College and Superspeciality Hospital, Sanathnagar, Hyderabad, Telangana, India. The hospital records of children with LMs who underwent injection sclerotherapy (ST) with aqueous bleomycin were analyzed retrospectively. Age, gender, presenting symptoms, physical findings, imaging, treatment methods, complications, duration of hospitalization, and outcome were noted. The diagnosis was based on physical examination findings in and ultrasonography (USG) with Doppler. Only those with macrocystic appearance on USG were included. All children underwent ST on an inpatient basis under USG guidance with informed parental consent. ST was performed using aqueous bleomycin 0.5 IU/kg per dose not exceeding five doses spaced 4 weeks apart. Sedation was used in children less than 5 years of age. After USG-guided site marking, the area was cleaned with povidone–iodine and covered with a sterile drape. The cyst was punctured with a 22G needle, all the fluid was aspirated, and diluted aqueous bleomycin (concentration 0.2–0.5 IU/mL) was instilled into the cyst volume equal to that of the aspirated fluid but not exceeding 20 mL. Compression dressing was applied for coaptation of cyst walls for 24 h after injection. Babies were kept in hospital for 24 h to monitor immediate reactions such as erythema, fever, pain, and so on. USG was repeated prior to next dose (after 4 weeks). Complete or near total disappearance of the lesion was considered an excellent response, regression of more than 50% of lesion size was considered a good response, and regression of less than 50% or no regression was considered poor response. Recurrence was defined as the regrowth of lesions after treatment. Parental satisfaction with cosmesis was recorded as excellent, good, and poor. Descriptive statistics were used to tabulate data.
RESULTS
Our study included 26 children with macrocystic non-visceral LMs. The age range was from 2 months to 168 months with a median age of 24 months. There were 18 male and 8 female children. Weight of the children ranged from 4 to 38 kg with a median of 12 kg. Table 1 shows the locations of the LMs in our study. Only one child (3.8%) in our study had multiple LMs (chest wall and left arm). The largest dimension of the LM on USG measurement ranged from 1 to 13 cm with a median of 3.5 cm. The median number of injections given was 2 (range 1–4).
| Site | Number (n=27)* |
|---|---|
| Neck | 10 (37%) |
| Chest wall | 7 (25.9%) |
| Upper arm | 5 (18.5%) |
| Axilla | 3 (11.1%) |
| Face | 1 (3.7%) |
| Abdominal wall | 1 (3.7%) |
*One child had two sites involved
The reduction in the size of the mass usually took between 14 and 90 days (median = 60 days). The median duration of follow-up after last ST has been 6 years (range 1–7 years). An excellent response was seen in 23/26 (88.4%) patients [Figures 2 and 3]. Three (11.5%) patients showed a good response to therapy [Figures 4 and 5] and achieved >50% reduction in size of their lesions with no cystic component left on USG. Only one of these underwent surgical excision of the residual in the chest wall for cosmesis, which showed only fibrosis on histopathology. The parents of the remaining two children did not want surgery for the residual fibrosis. No child (0%) had poor response to ST. Nine (34.6%) patients showed complete response with a single injection. No patient (0%) developed recurrence. Three (11.5%) children had minor complications: 2 developed fever on day 1 which subsided with non-steroidal anti-inflammatory drugs and 1 developed mild hypopigmentation of the overlying skin which is non-progressive at 6 years of follow-up. None of the patients developed any major complications till their last follow-up. Parental satisfaction was excellent in 24/26 (92.3%) and good in 2/26 (7.7%) patients.

- Complete or near total disappearance of the lesion was considered an excellent response seen in these children after aqueous bleomycin sclerotherapy
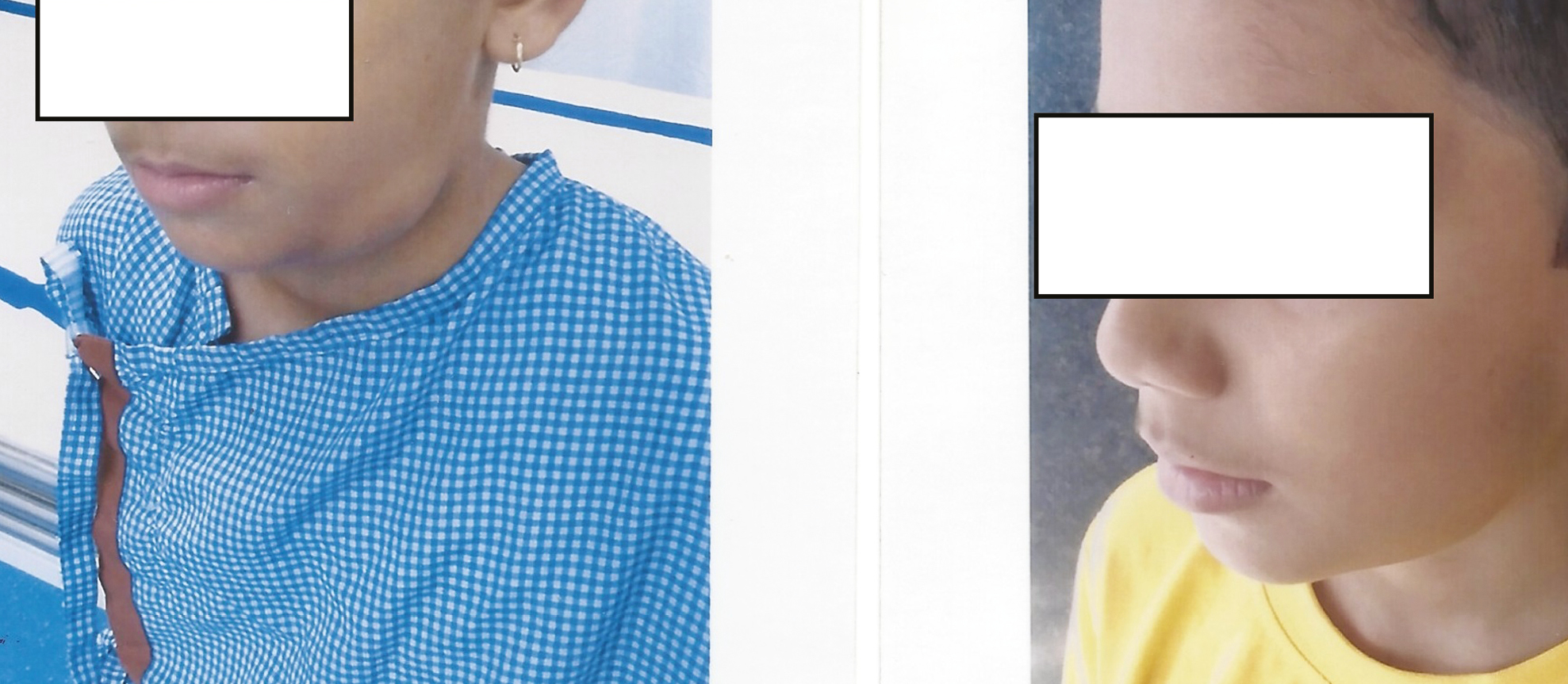
- Complete or near total disappearance of the lesion was considered an excellent response seen in these children after aqueous bleomycin sclerotherapy

- Regression of more than 50% of lesion size was considered a good response seen in these children after four and two doses of intralesional bleomycin, respectively, with no cystic component left on ultrasonography
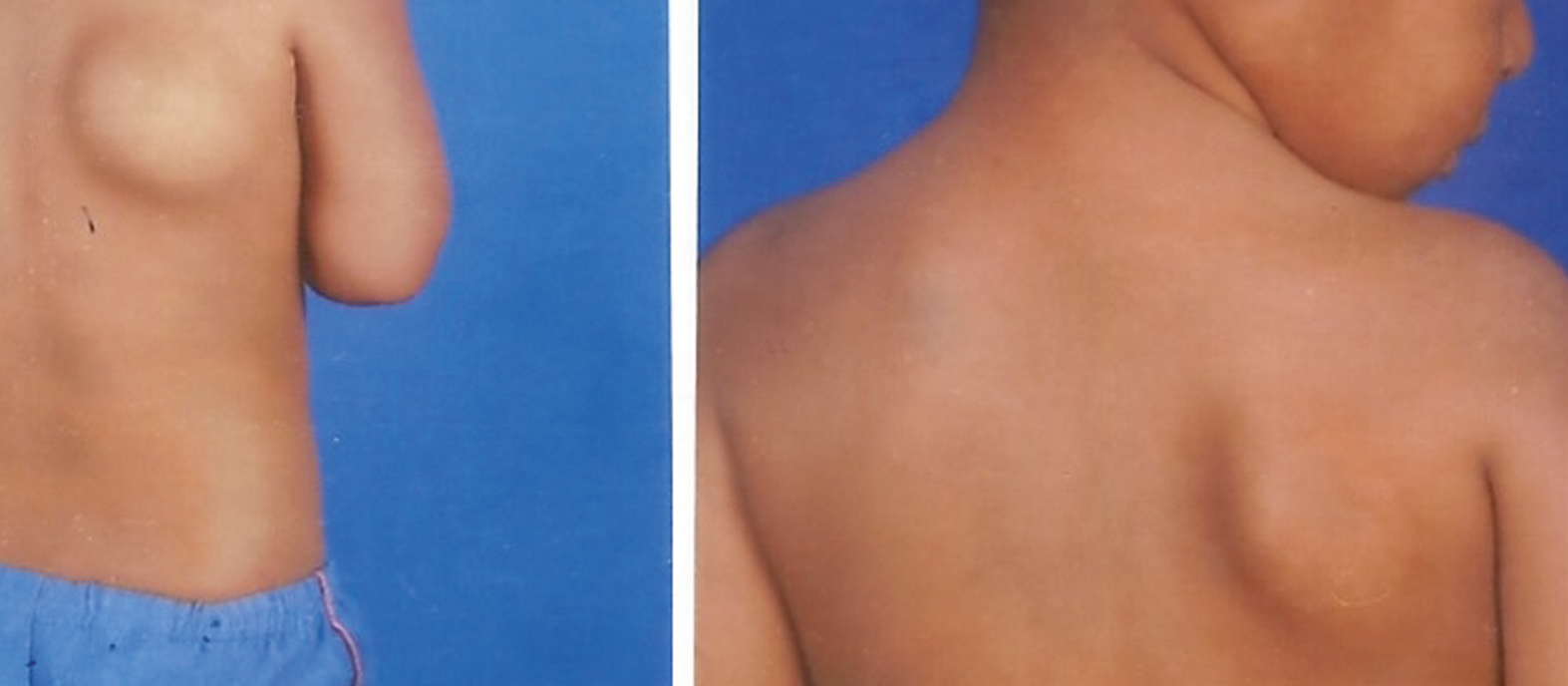
- Regression of more than 50% of lesion size was considered a good response seen in these children after four and two doses of intralesional bleomycin, respectively, with no cystic component left on ultrasonography
DISCUSSION
LMs comprise 5% of all vascular malformations typically characterized by no vascular flow on ultrasound Doppler. LMs are seen at birth in 60% of cases and in 80–90% cases by 2 years of age.[6] Rather than classifying lesion as macrocystic and microcystic based on the size of lesion, cysts which can be successfully aspirated and sclerosed resulting in decrease in the size of the lesion are considered significant.[7] Surgical excision can be associated with complications and morbidities in view of extensive dissection required causing disfigurement and poor cosmesis. Many lesions are characterized by infiltration of surrounding structures including vessels and nerves. Surgical excision is also associated with high rate of recurrence.[8910] In view of this alternate treatment, options were considered. One such modality is injection sclerotherapy. Many agents were tried historically, but majority caused unpredictable fibrosing response of the surrounding tissues causing difficulties in surgical excision if needed after sclerotherapy.[11]
Umezawa introduced bleomycin as an antitumor agent in 1966. In addition to inhibition of DNA synthesis, bleomycin was shown to produce a sclerosing effect due to its direct action on the endothelial cells producing a non-specific inflammatory reaction.[1213] This sclerosing effect was therapeutically used by Yura et al.,[5] in treating eight cystic hygroma patients by intralesional bleomycin injection in 1977. Their success led to further similar studies with encouraging results.[14151617]
Lipid-based bleomycin solution was used with good results because the solution retained for longer period in the lesion, thus maximizing its effect. But these are not easily available and expensive.[1114,18] Aqueous solution of bleomycin is easy to prepare, and multiple studies are published regarding the effect of aqueous bleomycin in LMs.[1118] Desired effect of sclerosis is achieved by local action of bleomycin, which depends on availability of drug per unit surface area of lesion.[19] Horbach et al.[12] published a systematic review and meta-analysis of the effect of intralesional bleomycin in venous malformations, in which the efficacy was good and the adverse event rate of bleomycin is significantly lower compared with the other sclerosants. Other vascular sclerosants, such as polidocanol and ethanol, act intralesionally and perilesionally, causing inflammatory reaction not only in the cyst but also in the surrounding normal tissue. Hence, chances of cosmetic deformity, i.e., cutaneous scarring and skin necrosis along with damage to vital structures such as facial nerve and parotid duct, can be much more when compared with bleomycin sclerotherapy.[12]
One of the described adverse effects of bleomycin is pulmonary toxicity, which is dose-dependent. If cumulative dose exceeds 400 IU or a single dose exceeds 30 U/m2 body surface area, then the risk of pulmonary toxicity increases. The risk further increases in elderly and in those who have underlying pulmonary disease.[19] However, our study and similar studies did not encounter any pulmonary complications, in which the dosage of bleomycin used was very low (maximum 0.5 IU/kg/dose with cumulative dose not exceeding 2.5 IU/kg).[4]
Similar to Bhatnagar et al.,[18] in our study, 88.4% of the cases had complete resolution of which 34.6% had complete response with a single injection. Our excellent response can be attributed to targeted drug delivery under ultrasound guidance, use of sedation wherever required to prevent child movement due to anxiety, pain, etc. and to post-procedure compression bandage which increased the contact time between the cyst wall and bleomycin.
In conclusion, intralesional bleomycin sclerotherapy is a safe non-surgical intervention for macrocystic pediatric lymphangiomas with reasonably good outcomes and even better parental satisfaction. Aqueous bleomycin is an efficacious and safe sclerosing agent for pediatric LMs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- New treatment options for lymphangioma in infants and children. Ann Otol Rhinol Laryngol. 2002;111:1066-75.
- [Google Scholar]
- Other vascular anomalies. In: Coran A, ed. Pediatric Surgery (7th ed.). Philadelphia: Mosby; 2012. p. :1613-30.
- [Google Scholar]
- Percutaneous sclerotherapy in neonatal and infant head and neck lymphatic malformations: A single center experience. J Pediatr Surg. 2011;46:2083-95.
- [Google Scholar]
- Bleomycin treatment for cystic hygroma in children. Nihon Geka Hokan. 1977;46:607-14.
- [Google Scholar]
- Slow-flow vascular malformations. In: Mulliken JB, Burrows PE, Fishman SJ, eds. Mulliken and Young’s Vascular Anomalies: Hemangiomas and Malformations (2nd ed.). New York: Oxford University Press; 2013. p. :562-94.
- [Google Scholar]
- Noninterventional treatment of selected head and neck lymphatic malformations. J Pediatr Surg. 2008;43:869-73.
- [Google Scholar]
- Percutaneous ethanol sclerotherapy for vascular malformations in the head and neck. Arch Facial Plast Surg. 2005;7:322-5.
- [Google Scholar]
- Cystic hygroma of the head and neck—A long-term follow-up of 44 cases. Acta Otolaryngol Suppl. 2000;543:248-50.
- [Google Scholar]
- Non surgical management of cystic lymphangioma. Indian J Otolaryngol Head Neck Surg. 2006;58: 355-7.
- [Google Scholar]
- Intralesional bleomycin injections for vascular malformations: A systematic review and meta-analysis. Plast Reconstr Surg. 2016;137:244-56.
- [Google Scholar]
- Bleomycin induces endothelial mesenchymal transition through activation of motor pathway: A possible mechanism contributing to the sclerotherapy of venous malformations. Br J Pharmacol. 2013;170:1210-20.
- [Google Scholar]
- Sclerosing therapy with bleomycin emulsion for lymphangioma in children. Pediatr Surg Int. 1990;5:270-3.
- [Google Scholar]
- Injection of bleomycin as a primary therapy of cystic lymphangioma. J Pediatr Surg. 1992;27:440-3.
- [Google Scholar]
- Efficacy of bleomycin treatment for symptomatic hemangiomas in children. Pediatr Surg Int. 1997;12:526-8.
- [Google Scholar]
- A new treatment with bleomycin for complicated cutaneous hemangioma in children. Eur J Pediatr Surg. 1997;7:158-62.
- [Google Scholar]
- Aqueous intralesional bleomycin sclerotherapy in lymphatic malformation: Our experience with children and adult. Natl J Maxillofac Surg. 2017;8:130-5.
- [Google Scholar]
- Goodman and Gilman’s The Pharmacological Basis of Therapeutics (10th ed.). New York: McGraw-Hill; 2001. p. :1430-57.




