
Translate this page into:
Esthetic importance of parietal eminence area (posterior parietal triangle), an essential island of scalp requiring hair restoration
*Corresponding author: Anil Kumar Garg, MS.MCh, MA (Yoga), ABHRS, FISHRS, CEO--Rejuvenate Plastic and Hair Transplant Centre, Indore, Bhopal, Madhya Pradesh, India. anilgarg61@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Garg AK, Garg S. Esthetic importance of parietal eminence area (posterior parietal triangle), an essential island of scalp requiring hair restoration. J Cutan Aesthet Surg. doi: 10.25259/jcas_14_22
Abstract
Hair loss is a progressive disorder, and if not treated in the early stages, it may lead to baldness, requiring a hair transplantation. Hair restoration of the frontal area of the scalp, followed by mid-scalp and vertex, is the usual preferential order of hair transplantation. Patients who underwent hair transplant in frontal and mid-scalp, because of the progressive nature of hair loss, later on showed prominent scalp show in parietal eminence area( posterior parietal triangle). This thinning in parietal eminence is noticeable in front and in the face’s lateral profile( side view), which is a concern to the patient. The parietal eminence or posterior parietal triangle is part of the vertex/crown, and the vertex is the last priority of scalp hair restoration. The author feels the parietal eminence area shall be transplanted while implanting the mid-scalp.
Keywords
Parietal eminence
Posterior parietal triangle
Occipitoparietal area

INTRODUCTION
Androgenetic alopecia (AGA)1 is one of the common causes of hair loss in men. The usual presentation is receding of the anterior hairline (AHL) with loss in the frontotemporal area of the scalp.2 When hair loss further progresses, it leads to hair loss in the parietal and occipital area leading to a drop-down of the parietal hump.3 The usual priority of reconstruction is the frontal area, followed by mid-scalp and crown.4 Due to the limitation of donor hair follicle supply, the temporoparietal region remains uncovered or minimally covered.4,5 The cases where the author did the transplant in the frontal, and mid-scalp, and noticed that the patient often complained of scalp show over the parietal eminence area, and widening of the part line which looks apparent in his side view.6 Hence, the author believes that the parietal eminence is one of the essential islands of the scalp, and there is a need to transplant the parietal eminence. It is advisable to include parietal eminence as an extension of the mid-scalp area, especially in cases where the possibility of going in a higher grade of baldness and or area showing thinning. After this study, the author started covering both sides of parietal eminences while covering the mid-scalp area.
Hair transplantation of the parietal eminence is an underappreciated means to maintain balance in the frontal and lateral profiles and restore the skull’s contours. In limited donor availability, preferential attention to parietal eminence or posterior parietal triangle transplant can benefit indirect vertex coverage.
Objective
Hair transplantation of the parietal eminence area (posterior parietal triangle) to maintain the patient’s esthetic look.
ESTABLISHED TECHNIQUES AND SHORTCOMINGS
Methodology
The patients were selected who had undergone a hair transplant and now showing thinning and or baldness in the parietal eminence area ( posterior parietal triangle).
The author examined his few hair transplant cases for the frontal and mid-scalp areas. Some of these patients showed thinning and or baldness in the parietal eminence area, which looked prominent in the lateral profile and even front view of these patients [Figure 1]. The compromised aesthetics of the scalp inspired the author to look at all his previously transplanted cases. He concluded that the parietal eminence area should also undergo hair transplantation as a mid-scalp to treat the future balding in the parietal eminence area.
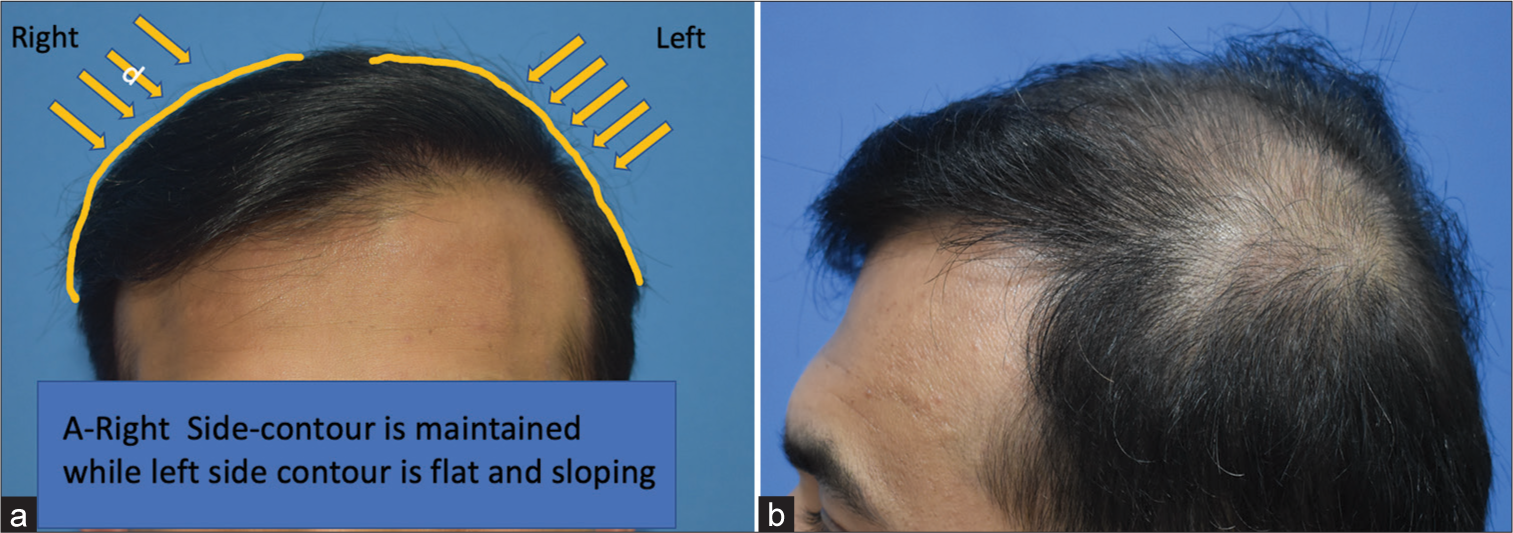
- Results after 11 months of hair transplant, whose (a) front and (b) mid-scalp were transplanted, now showing loss of contour on his left side and thinning in the parietal area and part line.
Modification in the plan to cover parietal eminence
Anteriorly, the mid-scalp area is bounded by an imaginary line connecting both the tragus, laterally on both sides of parietal humps, and posteriorly by the vertex transition point.7 Parietal eminence or posterior parietal triangles are part of the vertex area, as shown in Figure 2. If we look from the side profile of a face, the posterior parietal triangle/parietal eminence area shadows the central vertex area, and the central vertex area is visible only in the posterior profile of the scalp.
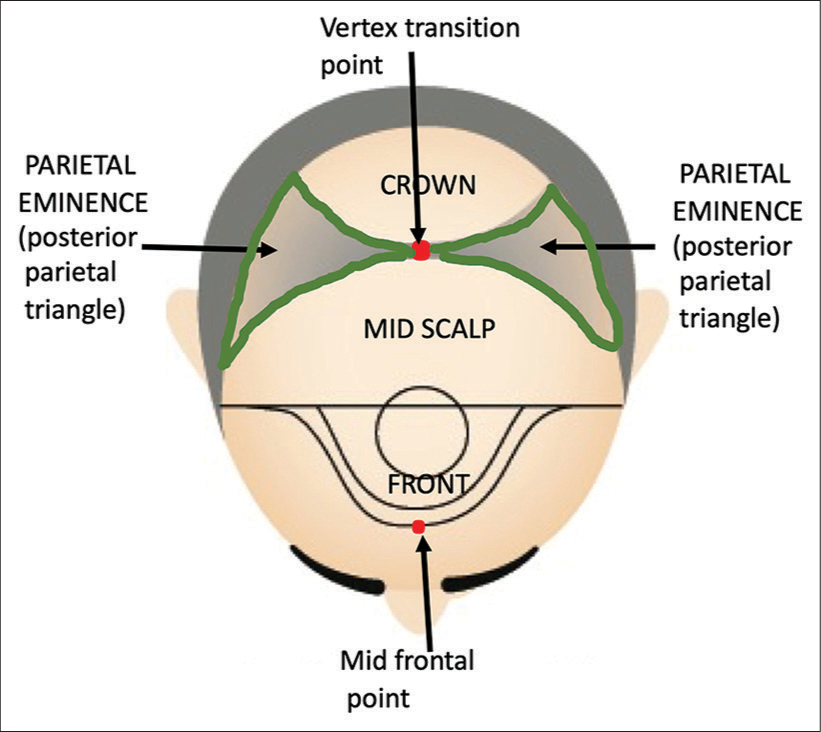
- Scalp major zones and posterior parietal triangles or parietal eminence areas.
Usually, the posterior parietal triangles are not covered during implantation in the mid-scalp area. The author proposes implanting the same number of donor follicles in the mid-scalp; we can reduce the mid-scalp area in the posterior midline zone by advancing the area of transplant anteriorly and extending both sides laterally to transplant the parietal eminence area, as shown in Figure 3. The same number of donor hair follicles covers both sides of parietal eminence/posterior parietal triangles. These modifications make the recipient area’s posterior border heart-shaped, as shown in Figure 3. If thinning is noticed in the part line, grafts are also implanted in the part line area.
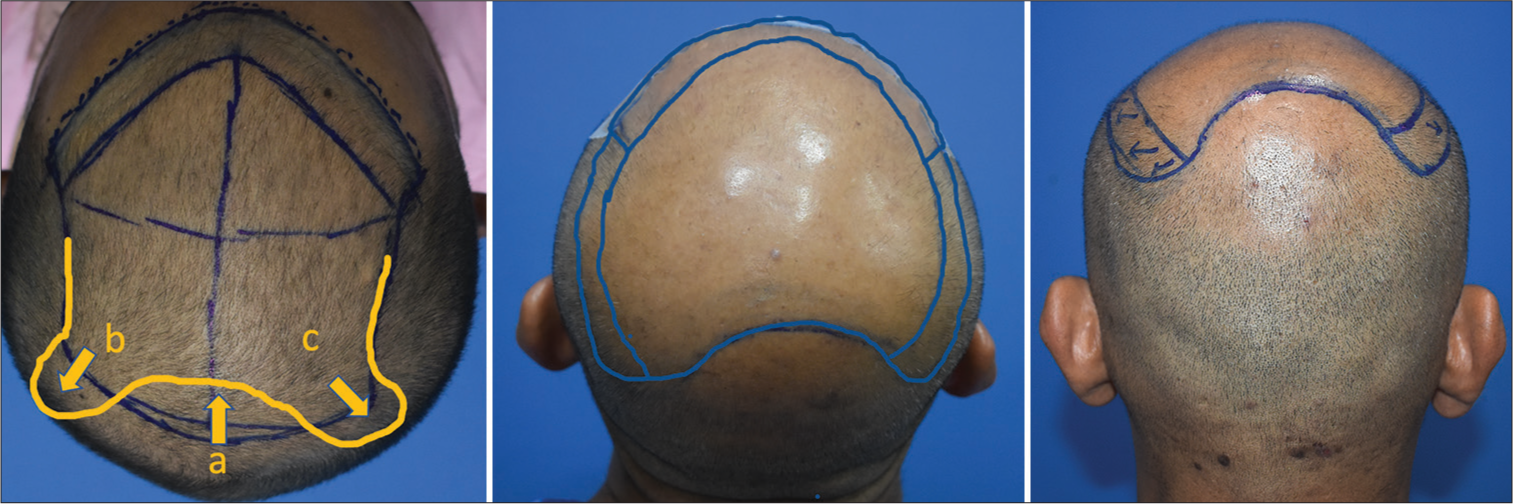
- Modification to cover posterior parietal area by extending posteriorly laterally in areas “b” and “c.” The final area looks like a heart shape.
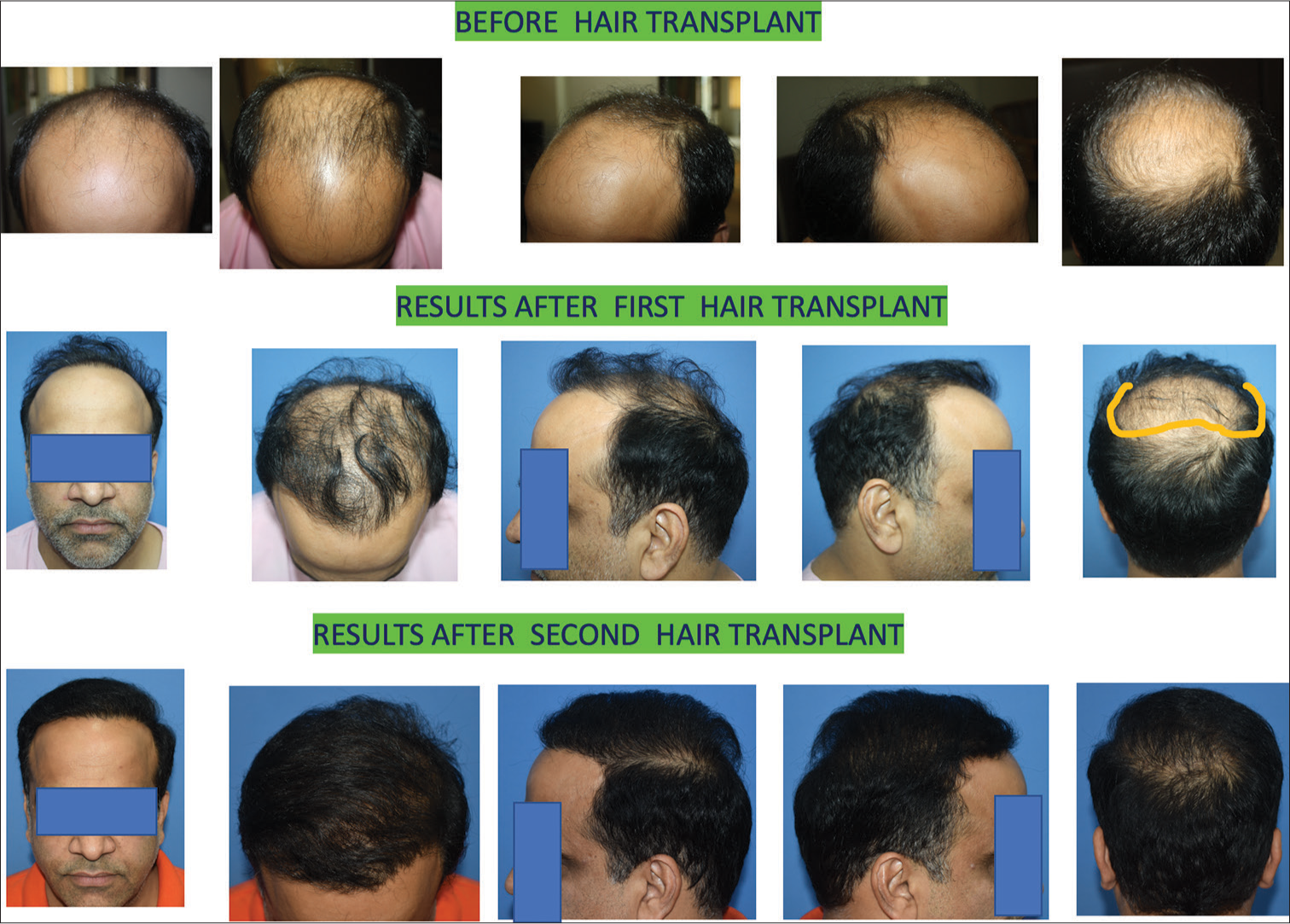
The author usually does 4500–5000 grafts in Norwood grade V to VII in the first stage of hair transplantation.2,8 Day one 2500–3000 grafts are harvested from the scalp using follicular unit extraction (FUE), and around 2000 grafts from the beard is extracted.8 First day all scalp hair follicles are implanted all over the planned area, leaving gaps between for beard grafts. On the 2nd day, donor hair follicles are harvested from the beard. The beard follicles are implanted between the scalp hair follicles which were implanted a day before, using the combination grafting technique of scalp and body hair.9 Author uses autologous plasma as graft holding solution.10 The areas transplanted are frontal, mid-scalp, and parietal eminence areas (posterior parietal triangle) as per the plan shown in Figure 3. They cover the frontal and mid-scalp areas with extension to parietal eminence on both sides. Figures 4-6 shows few cases ,where the parietal eminence was transplanted.

- This young man had hair loss and thinning in the front, mid-scalp and crown. A total of 5256 grafts were implanted in two days. On day one, three thousand thirty grafts were harvested from the scalp and 2226 grafts from the beard on the second day. Front, mid-scalp, including parietal eminence (posterior parietal triangle), were transplanted. After eight months of hair transplant, the results showed good coverage over parietal eminence.
- This young man Norwood grade VII. Follicular unit transplantation (FUT) was done. A total of 3506 grafts were implanted. After six years of primary hair transplant, a total of 4550 grafts were harvested, 2526 from the scalp by follicular unit extraction (FUE) and 2024 from the beard. The anterior hairline was revised, and mid-scalp and upper crown, including side parietal eminence areas, were transplanted. After ten months of hair transplant, the results showed good coverage, except lower crown area.

- This young man had Norwood grade VI baldness. Some surgeons implanted approximately 2500 follicular unit transplantation (FUT) grafts. However, the patient was concerned about thinning in the part line and parietal eminence area, which were quite noticeable in oblique and lateral profile. We implanted 5023 grafts from the scalp and beard, covering the parietal area and part of the crown. The results are after 13 months of hair transplant.
RESULTS
Case I
This young man had hair loss and thinning in the front, mid-scalp, and crown. A total of 5256 grafts were implanted in 2 days. On day 1, 3030 grafts were harvested from the scalp and 2226 grafts from the beard on the 2nd day. Front, and mid-scalp, including parietal eminence (posterior parietal triangle), were transplanted. After 8 months of hair transplant, the results showed good coverage over parietal eminence [Figure 4].
Case II
This young man is Norwood grade VII. Follicular unit transplantation (FUT) was done. A total of 3506 grafts were implanted. After 6 years of primary hair transplant, a total of 4550 grafts were harvested, 2526 from the scalp by FUE and 2024 from the beard. The AHL was revised, and the mid-scalp and upper crown, including side parietal eminence areas, were transplanted. After 10 months of hair transplant, the results showed good coverage, except lower crown area.
Case III
This young man had Norwood grade VI baldness. Some surgeons implanted approximately 2500 FUT grafts. However, the patient was concerned about thinning in the part line and parietal eminence area, which were quite noticeable in the oblique and lateral profile. We implanted 5023 grafts from the scalp and beard, covering the parietal area and part of the crown. The results are after 13 months of hair transplant.
DISCUSSION
The esthetics of the face lie in maintaining the proportion of one body part to another, bilateral symmetry, and contour of the face and scalp.2,8 The AHL, temporal fringe, maintains the framing of the face and proportion of facial parts, while the hair volume maintains the contour of the scalp all around the scalp.11
In balding males due to AGA, there is receding of the AHL, followed by temporal area recession and loss of hair bulk in the parietal and crown area. The restoration of the AHL is the first priory of hair restoration, followed by mid-scalp and, lastly, the crown. Thinning and loss of hair in the parietal and crown area leads to loss of scalp contour, leading to compromised esthetics. The parietal eminence is the most projecting part of the scalp, visible in the front, oblique, and lateral profiles. The loss of hair in this zone looks very prominent in the oblique and lateral profile of the face. The author has examined his cases, whose front and mid-scalp were restored, but most of the patients were concerned about the thinning and baldness in the parietal eminence area and wanted to cover it. The author feels that the restoration of parietal eminence shall be done during mid-scalp restoration.
Coverage of the parietal eminence is an underappreciated means to maintain balance in the frontal and lateral profiles and restore the skull’s contours. In situations of limited donor availability, preferential attention to parietal coverage can benefit indirect vertex coverage.
LEARNING POINTS
The parietal eminence is the most prominent part of the scalp, visible from the front, oblique, and lateral profiles.
Hair loss in this area is particularly noticeable from the oblique and lateral profiles of the face.
Upon analyzing cases of scalp transplants, the author suggests that restoration of the parietal eminence should be incorporated during mid-scalp restoration.
The author recommends reducing coverage in the posterior mid-zone of the mid-scalp and reallocating grafts to expand coverage on both sides of the mid-scalp to include the parietal eminence. This method optimizes graft usage.
This approach offers a graft-economical method for indirectly covering the vertex.
CONCLUSION
AGA is a progressive disorder. A young male with a positive family history has a very high chance of having a high grade of baldness. When transplanted in the frontal and mid-scalp area, any such patient is likely to develop soon thinning and or baldness in the nearby area like parietal eminence and parietal-occipital area, which looks prominent in his side profile, and he often does not like this.
After a study of many such cases on follow-up, the author has concluded that while transplanting the mid-scalp area of such patients, the parietal eminence and part line area shall be included in the mid-scalp area transplant the side profile of the patient looks balanced. Hence, the hair restoration of the parietal eminence area is one of the important aspects and it can benefit indirect vertex coverage in limited donor availability.
Authors’ contributions
The author conducted a comprehensive study of all cases operated upon, emphasizing the significance of parietal eminence coverage. Recognizing its crucial aesthetic role, the author developed a graft-economical method to effectively cover this important area while indirectly addressing vertex coverage. This modification in the transplant procedure significantly enhanced aesthetic outcomes using the same number of grafts.
Ethical approval
Institutional Review Board approval is not required as the study is a retrospective observational and analysis study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Classifications of patterned hair loss: A review. J Cutan Aesthet Surg. 2016;9:3-12.
- [CrossRef] [Google Scholar]
- Male and female pattern hair loss: Treatable and worth treating. Cleve Clin J Med. 2021;88:173-82.
- [CrossRef] [Google Scholar]
- Distribution of human hair in follicular units: A mathematical model for estimating the donor size in follicular unit transplantation. Dermatol Surg. 1999;25:294-8.
- [CrossRef] [Google Scholar]
- The use of body hair with scalp hair for “combination grafting” to enhance visual density of hair transplantation and increase coverage in advanced alopecia. Hair Transpl Forum Int. 2018;28:217-23.
- [CrossRef] [Google Scholar]
- Parietal eminence - Wikipedia. Available from: https://en.wikipedia.org/wiki/parietal_eminence [Last accessed on 2021 Dec 15]
- [Google Scholar]
- Follicular transplantation. Patient evaluation and surgical planning. Dermatol Surg. 1997;23:771-84. discussion 801-5
- [CrossRef] [Google Scholar]
- Donor harvesting: Follicular unit excision. J Cutan Aesthet Surg. 2018;11:195.
- [CrossRef] [Google Scholar]
- Combination grafting of scalp and body hair to enhance the visual density of hair transplant and coverage of higher grade of baldness. J Cutan Aesthet Surg. 2020;13:163.
- [CrossRef] [Google Scholar]
- A histological and clinical evaluation of plasma as a graft holding solution and its efficacy in hair growth and graft survival. Indian J Plast Surg. 2019;52:209.
- [CrossRef] [Google Scholar]
- Look at your hair the way you look at your face: Concept of total facial skin and hair care. Skin Appendage Disord. 2020;6:67-76.
- [CrossRef] [Google Scholar]




