
Translate this page into:
External Knot for Running Intradermal Stitch
Address for correspondence: Mr. Garrison Leach, Medical Student, Department of Surgery-Plastic Surgery, Creighton University School of Medicine, Phoenix, Arizona, USA. E-mail: GarrisonLeach@creighton.edu
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
We describe a unique method for closure of running subcuticular/intradermal suture that minimizes potential abscess formation and maximizes cosmetic outcomes.
Keywords
Surgery
suture
technique

INTRODUCTION
The standard technique for subcuticular/intradermal suturing entails placement of a buried knot at the distal apex of an incision, running the suture material with subcuticular/intradermal bites to the proximal apex where an additional buried knot is made, pulling the needle and suture material through the adjacent skin, and finally cutting it flush with the epidermis.[1]
Though this method is functionally reliable, there are several potential problems. One is that the buried knots are prone to abscess formation.[2] In addition, the bulk associated with the buried knots can leave a “dog-ear” appearance to the wound apices.[3]
Therefore, we present a technique in which the incision is closed without a buried knot mitigating the potential for abscess formation in addition to the cosmetically unappealing bulk at wound edges associated with standard subcuticular closure.
REPORT
The technique is articulated and shown in Figure 1 and Video 1. A standard intradermal bite at the distal apex is made leaving a long tail. Subsequent running intradermal bites are made from the distal to the proximal apex. When the proximal apex is reached, the needle and suture is brought out through the adjacent skin at a 90° angle. The suture is wrapped around the shaft of the needle driver. Using the needle driver, the suture is then grasped approximately 1cm from the skin [Figure 1A] Next, using the free, contralateral hand, the loop around the shaft is flipped over the jaws of the needle driver to create a knot with a loop [Figure 1B]. Attention is made to leave a slight air knot while securing the knot approximately 1cm above the skin. Additional throws are made using standard simple suture technique [Figure 1C]. After six total throws, the free end is cut [Figure 1D].
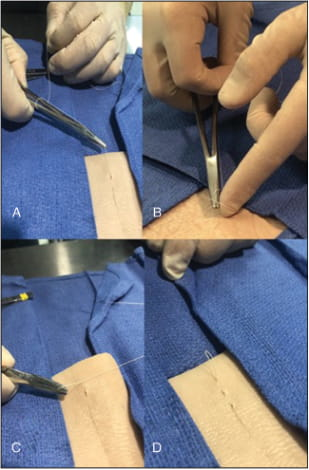
- (A–D) Steps for securing intradermal suture with external knot
CONCLUSION
We have seen outstanding functional and aesthetic results with this method. This technique is simple and reliable. It provides durability that is comparable to that with buried knots. Having the knot external mitigates the risk associated with granuloma and abscess formation posed by buried knots with the standard technique.[4567] Moreover, this technique maximizes cosmetic outcomes as the external knot minimizes the bulky, “dog-ear” appearance at the proximal apex commonly associated with the more common method of securement.[78]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
All videos available online www.jcasonline.com
REFERENCES
- Stitch granulomas following inguinal herniotomy: a 10-year review. J Pediatr Surg. 1993;28:1505-7.
- [Google Scholar]
- A simple technique for the retention of a subcuticular suture. Surgeon. 2003;1:149-51.
- [Google Scholar]
- Avoiding stitch abscesses in subcuticular skin closures: the L-stitch. Can J Surg. 2003;46:223-4.
- [Google Scholar]
- A technique for subcutaneous knot inversion following running subcuticular closures. Mil Med. 1992;157:255.
- [Google Scholar]
- Experimental studies in swine for measurement of suture extrusion. J Long Term Eff Med Implants. 2004;14:251-9.
- [Google Scholar]




