
Translate this page into:
Fractional Laser Resurfacing for Acne Scars: Our Experience at Tertiary Care Hospital of North India
Address for correspondence: Dr. Fozia Rehman, Department of Dermatology, Venereology & Leprosy, Government Medical College Srinagar, Srinagar 190010, Jammu and Kashmir, India. E-mail: drfoziarehman16@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
Acne is very common among adolescents, which may sometimes persist into adulthood, and acne scars continue to have a profoundly negative impact on quality of life. Of all the various modalities available, fractional lasers have shown effective results.
Aims and Objectives:
The aim of this study was to assess the efficacy and safety of fractional carbon dioxide (CO2) laser resurfacing in atrophic facial acne scars.
Materials and Methods:
The study included 104 subjects aged ≥18 years with atrophic acne scars on face of more than 6 months of duration recruited over a period of 1 year. All the patients were treated with fractional CO2 laser (600 W power and wavelength 10,600 nm). Four sessions of fractional CO2 laser resurfacing were done at 6-week intervals in each patient. We compared the improvement rate of scars after every session at 6-week interval, 2 weeks after the last session, and finally 6 months after the last laser session.
Results:
The difference between the mean baseline score (3.43) and mean final score (1.83) using Goodman and Baron’s qualitative scar scale was found to be statistically significant (P = 0.001). Mean improvement increased from first treatment session to the end of the treatment course from 0.56 to 1.62 indicating the role of the number of sessions in the overall improvement of acne scars. With regard to overall satisfaction, maximum number of patients were either very satisfied (55.8%) or satisfied (25%) as compared to those who were only slightly satisfied (11.5%) or completely unsatisfied (7.7%).
Conclusion:
Fractional ablative laser gives excellent results in the management of acne scars and has emerged as an appealing non-invasive option for this indication. Being a safe and effective option for atrophic acne scar treatment, it can be recommended wherever available.
Keywords
Ablative
acne-scars
fractional
laser

INTRODUCTION
Acne is a common skin disease though predominantly prevalent among teenagers. However, it continues to have a profoundly negative impact on quality of life in adulthood because of its most common and difficult to deal with complication, that is, scarring. The pathophysiology behind post-acne scarring is attributed to an altered wound healing response initiated by cutaneous inflammation, leading to an imbalance in matrix degradation and collagen biosynthesis which results in either excess or decreased collagen deposition ultimately leading to hypertrophic/keloid or atrophic acne scars, respectively. Atrophic scars account for around 75% of all acne scars and are further classified as ice-pick, boxcar, and rolled-over scars based on their shape and depth.[12]
There are many treatment options available to deal with acne scarring, such as topical retinoic acid application, chemical peeling, dermabrasion, scar revision/excision/subcision, punch grafting, skin rolling technique, fillers, intralesional injections, and ablative/non-ablative/ fractional resurfacing with lasers/lights/plasma devices.[13] Each treatment modality is best suited to deal with a particular type of acne scar, and each has its own risks and benefits. As more than one type of scar is commonly seen in an individual patient so a combination of procedures is often required to obtain the best results.[4] Energy-based devices primarily light/lasers and radiofrequency are currently emerging as the preferred treatment options not only for post-acne scarring but also for the treatment of active acne in view of being noninvasive and with minimal downtime as compared to the surgical ones.[56]
Facial resurfacing with fractional lasers (ablative––AFL and nonablative––NAFL) is nowadays considered to be one of the most effective treatment options for facial scars. Fractional lasers can be further subdivided into ablative and nonablative [Table 1] depending on their impact on stratum corneum. Ablative fractional lasers have wavelengths in the range of 2940–10,600 nm and lead to full-thickness destruction of skin, whereas nonablative fractional lasers have wavelengths ranging from 1320 to 1927 nm and leave a functionally and histologically intact stratum corneum compared to ablative fractional lasers.[789] Fractional lasers treat only a “fraction” or a column of the affected skin by microthermal zone (MTZ) formation, stimulating neocollagenesis and collagen remodeling leaving intervening areas of skin untreated. These untreated areas help in rapid re-epithelization of the skin, minimizing the chances of prolonged and serious adverse effects.[1011]
| Ablative lasers | Nonablative lasers | ||
|---|---|---|---|
| Nonfractional | Fractional | Nonfractional | Fractional |
| 10,600 nm CO2 | 10,600 nm CO2 | 1540 Er glass | 1550 nm Er:Doped |
| 2940 nm Er:YAG | 2940 nm Er:YAG | 1320 nm Nd:YAG | 1540 Er glass |
| 2790 nm Er:YSGG | 1064 nm Nd:YAG | 1440 nm Nd:YAG | |
| 1450 nm diode laser | 1927 nm thulium fiber | ||
| 755 nm alexandrite | 1927 nm Diode | ||
| 585 nm PDL | |||
| 595 nm PDL | |||
| 532 nm laser | |||
Fractional carbon dioxide (CO2) laser resurfacing combines the advantage of increased efficacy along with the safety of ablative laser with the benefit of reduced downtime associated with fractional laser. It has been used in the treatment of atrophic scars with varying degrees of success and the positive response achieved in previous studies has been attributed to the promotion of the wound healing process and amplified production of myofibroblasts and matrix proteins such as hyaluronic acid.[1213] Our study aims to assess the efficacy and safety of fractional CO2 laser treatment in the management of post-acne scars among patients attending tertiary care center.
MATERIALS AND METHODS
The study design was a hospital-based observational study to assess the efficacy and safety of fractional CO2 laser resurfacing in atrophic facial acne scars. The study protocol was approved by the institutional Ethical Committee. The study population included 104 subjects with atrophic acne scars recruited over a period of 1 year. Informed consent was obtained from each patient before enrolment.
Inclusion criteria included:
All patients aged 18 years and above with atrophic acne scars on face of more than six months duration.
Exclusion criteria included:
Active inflammatory acne for the last 6 months.
Concurrent skin inflammation/infection on the face.
Subjects who had a history of isotretinoin or hormonal use within 6 months before study treatment,
History of use of other physical modalities of scar treatments within the last 12 months.
History of keloidal tendency,
Pregnancy or lactation
Photosensitivity or recent use of photosensitizing medication.
Each patient was evaluated with respect to history and examination. In each patient, digital photographs were taken using a standard camera of 12 megapixel (MP) at baseline and the severity of acne scarring was estimated by Goodman and Baron’s qualitative acne scar grading system [Table 2].[14] Patients were asked about their rate of satisfaction at the final visit, and they were classified into very satisfied, only satisfied, slightly satisfied, or completely unsatisfied. Photographs were repeated prior to laser treatment at each sitting using identical camera settings, lighting, and patient positioning. Four sessions of fractional CO2 laser resurfacing were done at 6-week intervals in each patient. We compared the improvement rate of scars after every session at 6-week interval. At each follow-up visit, the scar was photographed and assessed by 2–3 observers with aim of decreasing the observer bias. Response to treatment was finally assessed 2 weeks after the last session, and the last follow-up was done 6 months after the final treatment session.
| Grade | Level of disease | Characteristics | Examples |
|---|---|---|---|
| 1 | Macular disease | Erythematous, hyper- or hypopigmented flat marks visible to patient or observer irrespective of distance | Erythematous, hyper- or hypopigmented flat marks |
| 2 | Mild disease | Mild atrophy or hypertrophy that may not be obvious at social distances of 50 cm or greater and may be covered adequately by makeup or the normal shadow of shaved beard hair in males or normal body hair if extrafacial | Mild rolling, small soft popular |
| 3 | Moderate disease | Moderate atrophic or hypertrophic scarring that is obvious at social distances of 50 cm or greater and is not covered easily by make-up or the normal shadow of shaved beard hair but is still able to be flattened by manual stretching of the skin | More significant rolling, shallow “boxscar,” mild-to-moderate hypertrophic or opular scars |
| 4 | Severe disease | Severe atrophic or hypertrophic scarring that is obvious at social distances of 50 cm or greater and is not covered easily by make-up or the normal shadow of shaved beard hair in males or body hair (if extrafacial) and is not able to be flattened by manual stretching of the skin | Punched out atrophic (deep “boxscar”), “ice pick,” bridges and tunnels, gross atrophy, dystrophic scars significant hypertrophy or keloid |
After cleaning the treatment areas with a mild cleanser, a topical mixture of lidocaine 2.5%, and prilocaine 2.5% cream was applied under occlusion to the treatment area for one hour prior to each treatment session. All the patients were treated monthly with fractional CO2 laser (Cis F1 Sellas Primium CO2 Laser manufactured by DINONA, South Korea), with 600 W of power and a wavelength of 10,600 nm. Laser parameters used were as follows: spot density (PPA) 64; pattern scattered; energy 20–30 mJ/MTZ; spot size 300 μm/ MTZ; handpiece 80 μm–50 mm; pulse width 0.04 ms; and pulse repetition rate 10 kHz in the stamping mode. The number of passes varied from 2 to 3. The stamping technique is performed by forming a preset pattern of multiple MTZs on a skin region within a well-defined exposure area of the fixed hand-piece and then moving the hand-piece to another skin region and repeating this until the entire treatment area is covered. Laser pulses were placed adjacent to one another without overlapping, thereby preventing new scar formation. Ice packs were applied immediately after treatment to relieve the burning. As none of the subjects in our study had a history of active infection, so no prophylactic antibiotics, antiviral, or antifungal agents were prescribed. The patients were advised to cleanse the treated area gently with only tap water and to avoid the use of any topical cosmetic on the face for 1 week. A topical antibiotic-steroid cream was applied by patients for few days in case of more erythema and edema. Also, patients were instructed to avoid sun exposure and cosmetic application and to wear a broad-spectrum sunscreen two to three times a day. Adverse effects, if any, were also monitored at each follow-up visit.
Statistical analysis
All data were collected and transferred to Microsoft Office Excel. The statistical analysis was performed using Statistical Package for the Social Sciences software, version 19.0 (SPSS, Chicago, Illinois). Unpaired t test was used for statistical analysis and P values <0.05 were considered to be significant.
RESULTS
This study included 104 patients (39 males and 65 females). The age of patients varied from 19 to 45 years with a mean age of 28.49 ± 5.7 years. Most of the patients 65 (62.5%) were in the 3rd decade of life. The cases belonged to either Fitzpatrick skin type III or IV and were having moderate-to-severe atrophic post-acne scars according to Goodman and Baron classification system: 59 (56.7%) had grade 3 and 45 (43.2%) had grade 4 acne scars. According to morphologic types, the majority of patients 74 (71%) had mixed type of post-acne scars, 19 (18.2%) had predominantly rolling and boxcar type of scars, whereas 11 (10.5%) had a predominantly ice-pick type of scars. The commonest sites involved were the cheeks in 98 (94.2%) of patients, followed by the temples in 60(57.69%), forehead in 12 (11.5%), and chin was affected only in 3 patients (2.8%).
According to the physician assessment using Goodman and Baron’s qualitative acne scar grading system, response was seen in 100 (96%) cases, whereas there were 4 patients (3.8%) in which no response was noted. The response to the treatment in terms of decrease in grades in both groups of grade 3 and grade 4 according to Goodman and Baron’s qualitative acne scar grading system is given in tabulated form [Table 3]. The mean baseline score using Goodman and Baron’s qualitative scar scale was 3.43 ± 0.49 and mean final score 2 weeks after the last session was 1.83 ± 0.86, and the difference between the baseline and final scores was statistically significant (P = 0.0001) [Figures 1,2,3–4].
| Grade | Lesion | No. of patients | Post treatment reduction by 3 grades n (%) | Post treatment reduction by 2 grades n (%) | Post treatment reduction by 1 grades n (%) | No post treatment scar reduction n (%) |
|---|---|---|---|---|---|---|
| 1 | Macular | 0 | – | – | – | – |
| 2 | Mild | 0 | – | – | – | – |
| 3 | Moderate | 59 (56.7) | 0 (0) | 43 (72.8) | 15 (25.4) | 1(1.7) |
| 4 | Severe | 45 (43.2) | 3 (6.6) | 18 (40) | 21 (46.6) | 3(6.6) |
| Total | 104 | 3 (2.88) | 61(58.6) | 36(34.6) | 4 (3.84) | |
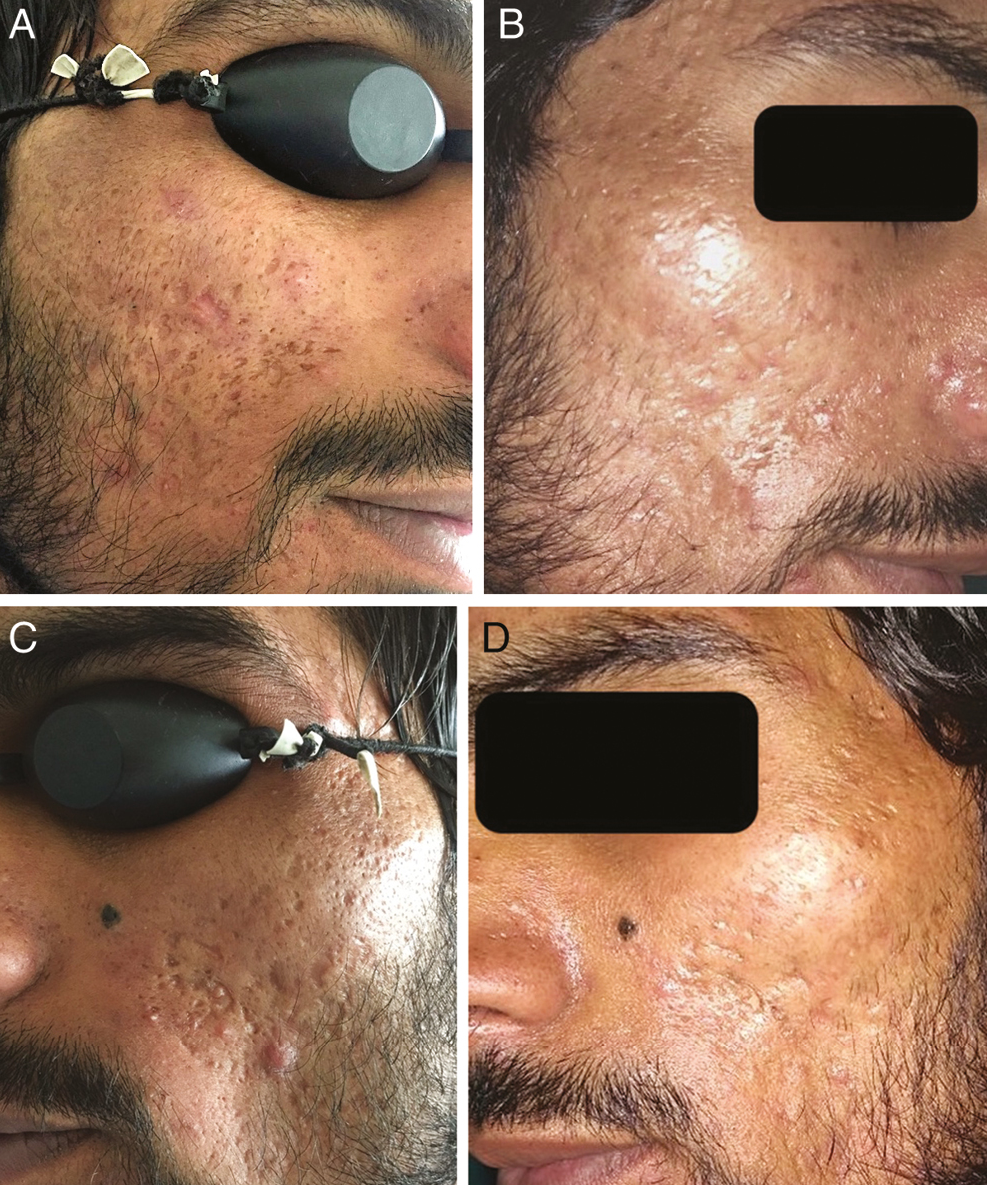
- (A) Acne scars over cheeks before treatment sessions. (B) Significant improvement in scarring seen following four sessions of fractional CO2 laser at 6 months. (C) Mixed types of scars over the cheek before treatment. (D) Significant improvement after treatment sessions

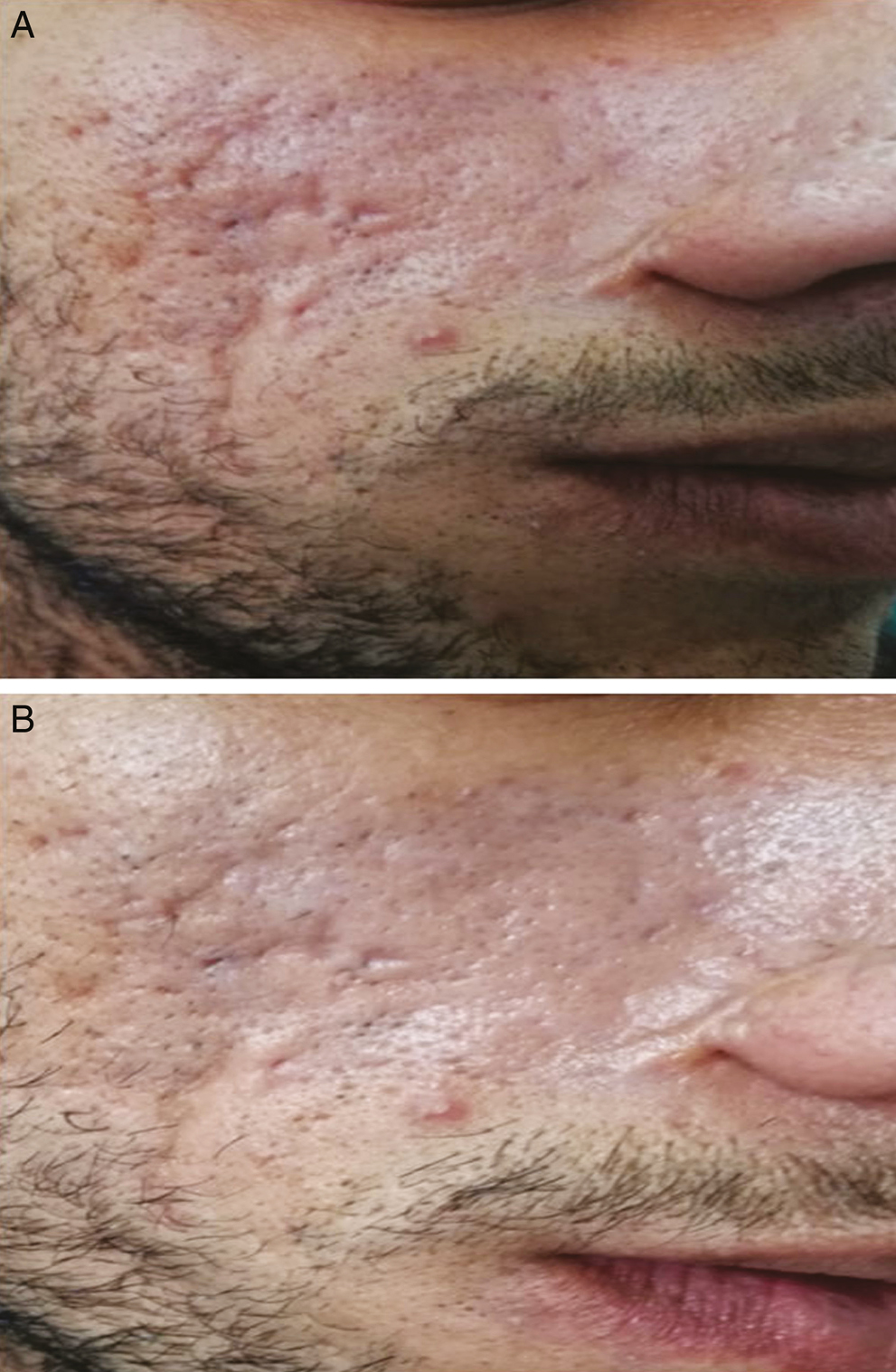
- (A) Rolling and boxcar scars over cheeks before treatment. (B) Improvement in scars after four sessions of fractional laser
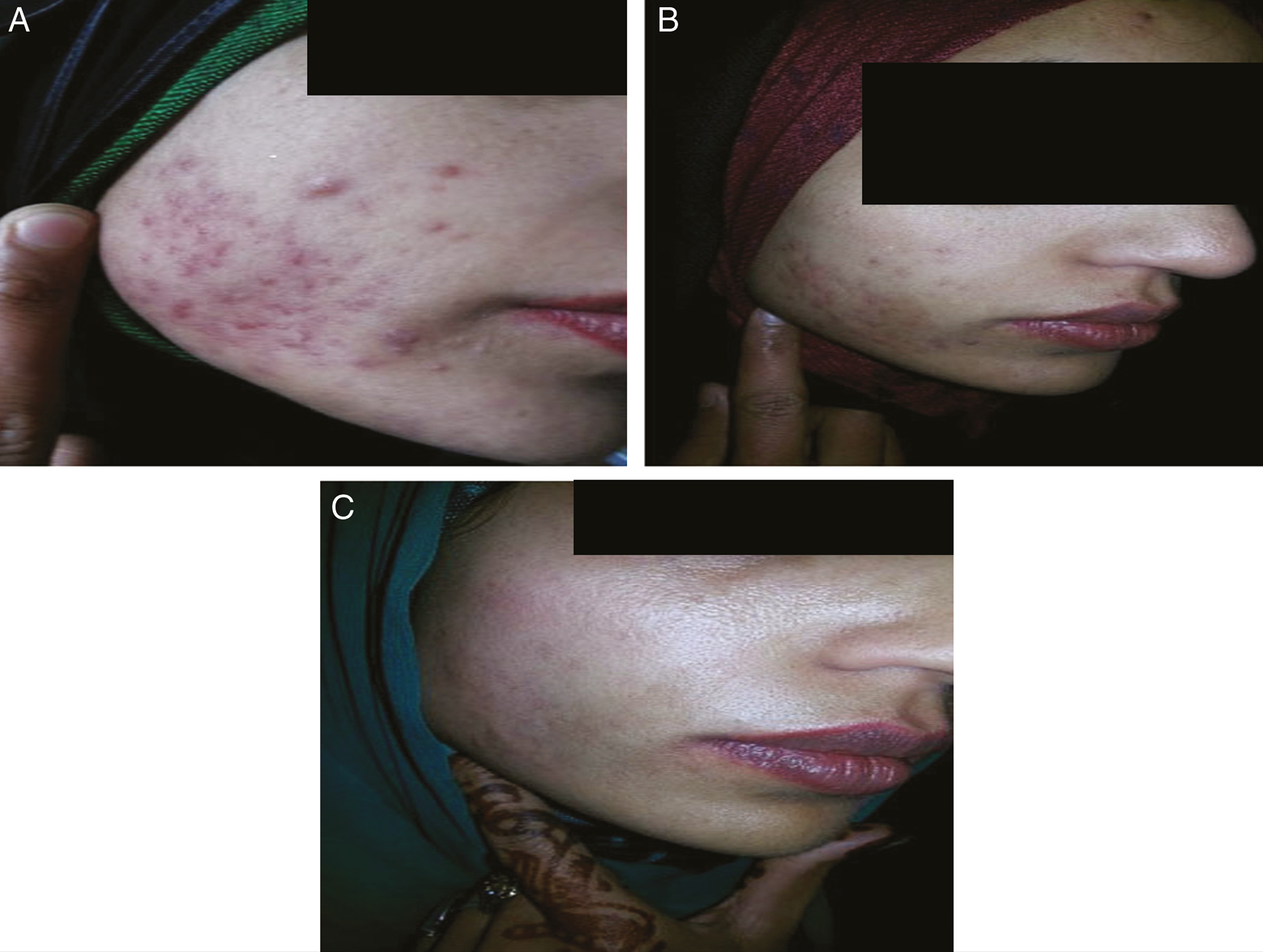
- (A) Acne scars over cheeks before laser sessions. (B) Improvement in scars after four sessions of fractional laser therapy. (C) Excellent response after 6 months of four sessions of fractional CO2 laser
- (A) Mixed types of scars over cheeks before treatment. (B) Mild response after four sessions of therapy
In our study, it was noted that the mean improvement increased from the first treatment session to the end of treatment course. Mean improvement score increased from 0.56 after 1st treatment session to 1.62 after four treatment sessions. It was also noted that the results attained in patient depends on the number of passes per session and number of sessions. The results found after the last session were found to be consistent even 6 months after the last session in 61 patients (58.6%) who returned for visit at 6 months. However, we did not calculate the score at end of 6 months as only 58.6% of cases were reported at follow-up visits.
Patient surveys with regard to overall satisfaction revealed that 58 (55.8%) were very satisfied, 26 (25%) were satisfied and 12(11.5%) were slightly satisfied at 2 weeks after the last session. For the remaining 8 cases, the improvement achieved was not up to their expectations. In our study, apart from mild and tolerable burning pain perceived by all cases (100%) during treatment session, only 32% cases reported other side effects and included transient mild erythema and edema, crusting, and scaling which settled in 2–3 weeks. Delayed pigmentation was seen in 12% of cases, which settled over a period of 6–8 weeks after advising broad-spectrum sunscreens and topical depigmenting agents.
DISCUSSION
Fractional ablative lasers have given excellent results in the management of acne scars which is a challenging cosmetic problem and has emerged as an appealing noninvasive option for this indication. Fractional CO2 laser, with a wavelength of 10,600 nm, has been employed in the treatment of acne scars in both Caucasian as well as Asian patients.[15161718]
In our study, all patients had grade 3 or 4 acne scars according to the Goodmann and Baron qualitative classification and at end of our study we could find a positive response in the majority of these patients. The mean baseline score using Goodman and Baron’s qualitative scar scale was 3.36 ± 0.49 and the mean final score was 2.7 ± 0.53, and the difference between the baseline and final scores was statistically significant (P = 0.0001) indicating excellent improvement in the quality of scars. Various studies conducted in the past have shown similar results though its role has not been documented in the Indian population to a great extent. Alster et al.[19] investigated the efficacy of fractional laser for facial atrophic acne scars in 53 patients. In their study, masked assessors reported a 25%–50% clinical improvement in 91% of patients after a single treatment. Mean clinical scores increased incrementally after each treatment with a 51–75% improvement noted in 87% of patients that received three treatments at 4-week intervals. The authors also concluded that fractional laser treatment showed a similar mild and limited side effect profile across all Fitzpatrick skin types. Chapas et al.[20] documented an improvement of 26%–50% in texture and atrophy of the skin in all patients in their study on facial acne scars and none of the enrolled patients developed any long-term or permanent adverse effects. Walgrave et al.[21] showed improvement in 23 out of 25 subjects having moderate/severe atrophic acne scars at 3-month follow-up after giving three sessions of fractional CO2 laser and noted transient side effects. Cho et al.[22] showed the efficacy as well as safety of fractional CO2 laser resurfacing in acne scars as they noted clinical improvement of >50% in 10 patients and 26%–50% improvement in 7 patients out of total 20 Korean subjects enrolled in their retrospective study. Manuskiatti et al.[23] showed 25% and 50% improvement in acne scar smoothness and volume 6 months after four treatment sessions in 13 Asian patients with Fitzpatrick skin type 4. Hedelund et al.[24] showed statistically significant improvement in skin texture and atrophy in comparison with placebo after 3 monthly laser sessions with fractional CO2 device using energies in the range of 48-56 mJ in 13 patients. Majid and Imran used laser as monotherapy in 60 Indian patients of atrophic acne scars in which excellent response was observed in 26 patients (43.3%), whereas 15 (25%) and 19 patients (31.7%) showed a good and poor response, respectively. Rolling and superficial boxcar scars responded the best, whereas pitted scars responded the least to fractional laser monotherapy.[25] In a study conducted by Ahmad et al.,[26] out of the 16 patients, two of the patients showed almost clearance of scarring (grade 4), whereas a large number (13 patients) showed mild to moderate healing of acne scars. An average improvement of 71% was observed. Saeed and Alsaiari[27] included 40 patients in their study in 2018 and showed a positive response with either good or excellent results in 30 patients.
It has been seen since previous experiences that the total number of laser sessions has an important role in the overall improvement in the scars observed at the end of treatment sessions. Similarly in our study the mean improvement after the first laser session at the first follow-up visit was 0.56 which increased up to 1.64 at the follow-up visit after the fourth session, thus further supporting the role of number of sessions in the overall treatment response. A significant improvement in acne scars has been shown after five 2940-nm erbium:YAG laser treatments sessions, whereas only mild to moderate improvement has been seen achieved after two treatments.[2829]
The increased improvement can be attributed to the cumulative effect of all treatment sessions and also to the continuing remodeling or neocollagenoses even after end of treatment sessions. It has been shown by few studies from the past revealing the role of use of single sitting of fractional laser in acne scars. Trelles et al.[30] used fractional CO2 laser device in a single sitting using medium to high setting depending upon skin type in total of 40 patients having atrophic acne scars and wrinkles. After 2 months, treatment has improved wrinkle aspect and scar condition, and no patient reported any adverse effects or complications, irrespective of skin type. Similar result in the improvement of acne scars has been shown by Hsiao et al.[31] where a single session of fractional CO2 laser was given to 25 patients with mild to moderate acne scars and showed that the mean grade of improvement in grade over baseline was 1.96 at 1 month and over 2.41 after 3 months, although eight patients did not return for follow-up at that point concluding that single treatment with CO2 fractional laser is effective for acne scars with minimal and acceptable side effects.
In our study laser parameters did not vary much from one patient to another, so we could not find the association between the different laser parameters and overall response however earlier studies have shown a high-fluence, low-density setting to be more efficacious than a low-fluence, high-density setting. Jung et al.[32] have conducted a split-face RCT of ablative CO2 Fractional photothermolysis (FP) and reported an improvement between 26% and 50% in six out of 10 patients on a low-fluence and high-density setting, whereas five out of 10 showed improvement of 76%–100% on a high-fluence and low-density setting. Similarly Mahmoud et al.[33] also compared two different settings (10 and 40 mJ) using a 1550-nm nonablative FP laser and the average scar improvement was 1.5 and 1.6, respectively, suggesting that higher fluence achieves better results.
In our study, results were assessed clinically and we did not subject the patients to invasive procedures of skin biopsy to show the histological effects of fractional laser therapy. However, studies in past based on both ablative and nonablative lasers have shown the histological effects of fractional lasers over skin.[1330,3435] Fibroblast-derived neocollagenesis is main factor responsible for the visible clinical results.[35] Apart from neocollagenesis, Yoo et al.[36] found an increase in the elastic fiber framework in the papillary dermis and new elastic fibers in the upper and mid-dermis, and the elastic fibers appeared to be well structured and less fragmented 12 weeks after the final treatment. Trelles et al.[30] showed a thicker, multicellular epidermis, a well-structured, fine keratin layer, and denser fibers at the dermis layer in their study using CO2 laser fractional resurfacing for acne scars.
In our study, apart from mild and tolerable burning pain perceived by all cases during treatment session, only few cases reported other side effects and included transient mild erythema and edema, crusting, and scaling which settled in 2–3 weeks. The most common side-effects of FP treatment reported earlier include erythema, edema, crusting and scaling, and occasionally there were cases of post-inflammatory hyperpigmentation (PIH), acneiform eruption, herpes infection, and dermatitis.[2337,38]
It is important to mention that the therapeutic varying results achieved with fractional laser resurfacing seen in different previously conducted clinical and histopathological studies may be attributed to variations in the types of scar treated, variations in energy sittings, total number of sessions, point of time of final assessment and lack of similar or uniform assessment tool. Despite the superiority and beneficial role of fractional ablative lasers, their use in Asian patients was discouraged earlier due to associated side effects and complications. However many authors postulate however that side effects can be minimized by selecting appropriate settings depending on patient skin type and properly following the manufacturer’s protocol.[39]
CONCLUSION
In conclusion, our study reiterates the observation that CO2 fractional laser is effective in treating atrophic acne scars with minimal side-effects and should be offered wherever this facility is available.
Limitations
It was a prospective study and no comparisons could be made with other modalities of treatment. No comparison was made between the response to different fractional laser parameters with respect to fluence and density. This study was not an observer/ evaluator-blinded study. The response of different types of scars to the treatment modality was not assessed separately.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Acne scars: Pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893080.
- [Google Scholar]
- Management of acne scars: Fulfilling our duty of care for patients. Br J Dermatol. 2015;172:47-51.
- [Google Scholar]
- Practical evaluation and management of atrophic acne scars: Tips for the general dermatologist. J Clin Aesthet Dermatol. 2011;4:50-7.
- [Google Scholar]
- Laser and other light therapies for the treatment of acne vulgaris: Systematic review. Br J Dermatol. 2009;160:1273-85.
- [Google Scholar]
- Light therapies for acne: Abridged Cochrane systematic review including GRADE assessments. Br J Dermatol. 2018;178:61-75.
- [Google Scholar]
- Cutaneous resurfacing with Co2 and erbium: Yag lasers: Preoperative, intraoperative, and postoperative considerations. Plast Reconstr Surg. 1999;103:619-32; discussion 633-4.
- [Google Scholar]
- Lasers in dermatology: Four decades of progress. J Am Acad Dermatol. 2003;49:1-31; quiz 31-4.
- [Google Scholar]
- The spectrum of laser skin resurfacing: Nonablative, fractional, and ablative laser resurfacing. J Am Acad Dermatol. 2008;58:719-37; quiz 738-40.
- [Google Scholar]
- Fractional photothermolysis: A new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34:426-38.
- [Google Scholar]
- Fractionation: A new era in laser resurfacing. Clin Plast Surg. 2011;38:449-61, vii.
- [Google Scholar]
- Laser treatment for facial acne scars: A review. J Cosmet Laser Ther. 2018;20:424-35.
- [Google Scholar]
- Increased smooth muscle actin, factor xiiia, and vimentin-positive cells in the papillary dermis of carbon dioxide laser-debrided porcine skin. Dermatol Surg. 1997;23:891-5.
- [Google Scholar]
- Postacne scarring: A qualitative global scarring grading system. Dermatol Surg. 2006;32:1458-66.
- [Google Scholar]
- Long-term efficacy of a fractional resurfacing device. Lasers Surg Med. 2010;42:168-70.
- [Google Scholar]
- Fractional ablative carbon dioxide laser resurfacing for skin rejuvenation and acne scars in Asians. Lasers Surg Med. 2010;42:615-23.
- [Google Scholar]
- Fractional ablative carbon dioxide laser in the treatment of atrophic acne scarring in Asian patients: A pilot study. J Cosmet Laser Ther. 2010;12:61-4.
- [Google Scholar]
- A new modality for fractional Co2 laser resurfacing for acne scars in Asians. Lasers Med Sci. 2013;28:627-32.
- [Google Scholar]
- The use of fractional laser photothermolysis for the treatment of atrophic scars. Dermatol Surg. 2007;33:295-9.
- [Google Scholar]
- Successful treatment of acneiform scarring with Co2 ablative fractional resurfacing. Lasers Surg Med. 2008;40:381-6.
- [Google Scholar]
- Evaluation of a novel fractional resurfacing device for treatment of acne scarring. Lasers Surg Med. 2009;41:122-7.
- [Google Scholar]
- The efficacy and safety of 10,600-nm carbon dioxide fractional laser for acne scars in Asian patients. Dermatol Surg. 2009;35:1955-61.
- [Google Scholar]
- Efficacy and safety of a carbon-dioxide ablative fractional resurfacing device for treatment of atrophic acne scars in Asians. J Am Acad Dermatol. 2010;63:274-83.
- [Google Scholar]
- Fractional Co2 laser resurfacing for atrophic acne scars: A randomized controlled trial with blinded response evaluation. Lasers Surg Med. 2012;44:447-52.
- [Google Scholar]
- Fractional Co2 laser resurfacing as monotherapy in the treatment of atrophic facial acne scars. J Cutan Aesthet Surg. 2014;7:87-92.
- [Google Scholar]
- Efficacy and safety of ablative fractional carbon dioxide laser for acne scars. J Pak Assoc Derma. 2017;22:41-4.
- [Google Scholar]
- Fractional CO2 laser resurfacing in the treatment of facial acne scars. Int J Med Sci Public Health. 2018;7:630-7.
- [Google Scholar]
- A 2940 nm fractional photothermolysis laser in the treatment of acne scarring: A pilot study in China. J Drugs Dermatol. 2009;8:978-80.
- [Google Scholar]
- Minimally ablative erbium:Yag laser resurfacing of facial atrophic acne scars in Asian skin: A pilot study. Dermatol Surg. 2008;34:681-5.
- [Google Scholar]
- Safe and effective one-session fractional skin resurfacing using a carbon dioxide laser device in super-pulse mode: A clinical and histologic study. Aesthetic Plast Surg. 2011;35:31-42.
- [Google Scholar]
- Efficacy and safety of a single treatment using a 10,600-nm carbon dioxide fractional laser for mild-to-moderate atrophic acne scars in Asian skin. Dermatologica Sinica. 2013;31:59-63.
- [Google Scholar]
- Lower-fluence, higher-density versus higher-fluence, lower-density treatment with a 10,600-nm carbon dioxide fractional laser system: A split-face, evaluator-blinded study. Dermatol Surg. 2010;36:2022-9.
- [Google Scholar]
- Safety and efficacy of erbium-doped yttrium aluminum garnet fractionated laser for treatment of acne scars in type Iv to Vi skin. Dermatol Surg. 2010;36:602-9.
- [Google Scholar]
- Pilot investigation of the correlation between histological and clinical effects of infrared fractional resurfacing lasers. Dermatol Surg. 2008;34:1443-53.
- [Google Scholar]
- Fractional photothermolysis: A novel aesthetic laser surgery modality. Dermatol Surg. 2007;33:525-34.
- [Google Scholar]
- The use of 1540 nm fractional photothermolysis for the treatment of acne scars in Asian skin: A pilot study. Photodermatol Photoimmunol Photomed. 2009;25:138-42.
- [Google Scholar]
- Adverse events of fractionated carbon dioxide laser: Review of 373 treatments. Dermatol Surg. 2010;36:1645-50.
- [Google Scholar]
- Fractionated laser skin resurfacing treatment complications: A review. Dermatol Surg. 2010;36:299-306.
- [Google Scholar]
- Fractionated Co2 laser resurfacing: Our experience with more than 2000 treatments. Aesthet Surg J. 2009;29:317-22.
- [Google Scholar]




