
Translate this page into:
Non-surgical Brachioplexy Using Polydioxanone Threads and Onabotulinum Toxin Type A in an Indian Female Patient: A Case Report
Address for correspondence: Dr. Shikha Bansal, Department of Dermatology and STD, VMMC and Safdarjung Hospital, Delhi, India. E-mail: contactshikha@rediffmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
Polydioxanone (PDO) threads have been used to improve face sag and laxity; however, they are seldom used for body laxity. Similarly, onabotulinum toxin type A has rarely been reported for intradermal use in skin tightening.
Materials and Methods:
We discuss use of PDO threads in combination with intradermal onabotulinum type A for the treatment of bilateral arm laxity after significant weight loss.
Results:
Bilateral skin laxity of arm was substantially corrected with two sessions of combination treatment with PDO threads and onabotulinum type A.
Conclusion:
A somewhat easy, significant, and effective technique leading to modest correction of arm laxity in this patient with PDO threads and onabotulinum toxin type A may suggest this method as an option for patients seeking non-surgical options with minimal downtime.
Keywords
Arm-lift
botulinum toxin A
brachioplexy
PDO threads

INTRODUCTION
Aesthetic arm contouring is often demanded. Surgical brachioplexy addresses this well; however, non-surgical options are often desired by patients. We present a novel combination therapy of PDO threads with onabotulinum A, improving skin laxity and texture of bilateral arms after weight loss.
CASE REPORT
A 58-year-old healthy female presented with sagging and laxity of bilateral upper arms following voluntary weight loss. The patient had minimal-to-moderate subcutaneous fat with minimal skin laxity and was categorized in stage 1 upper arm change. The classification is based on the arm contour scale, which is a surgical scale.[1]
This significant psychological stress warranted treatment to improve the condition. Surgical and non-surgical options were discussed with respective outcome. She opted for correction with onabotulinum A and PDO double screw 50 mm threads. A correction was achieved with a two-step approach at 14-day interval.
Technique
The medial arm skin is thinner than other body parts, prone to early wrinkling. The superficial fascial system described by Lockwood[2] supports the posteromedial arm as a sling and contiguous with clavipectoral and axillary fascia. This mechanism fails with aging or significant weight loss, causing ptosis of the posteromedial arm.
Thorough physical examination was done, including assessment of the entire circumference of the arms with arms abducted and elbows flexed at 90° obtaining maximal tissue relaxation. To identify the most depend area, the arm was held perpendicular to the long axis of the body, with the forearm at 90° to the humerus and palm facing anteriorly [Figure 1]. The soft tissue inferior to the bicipital groove was treated [Figure 2].

- Patient examination position to evaluate sag and laxity
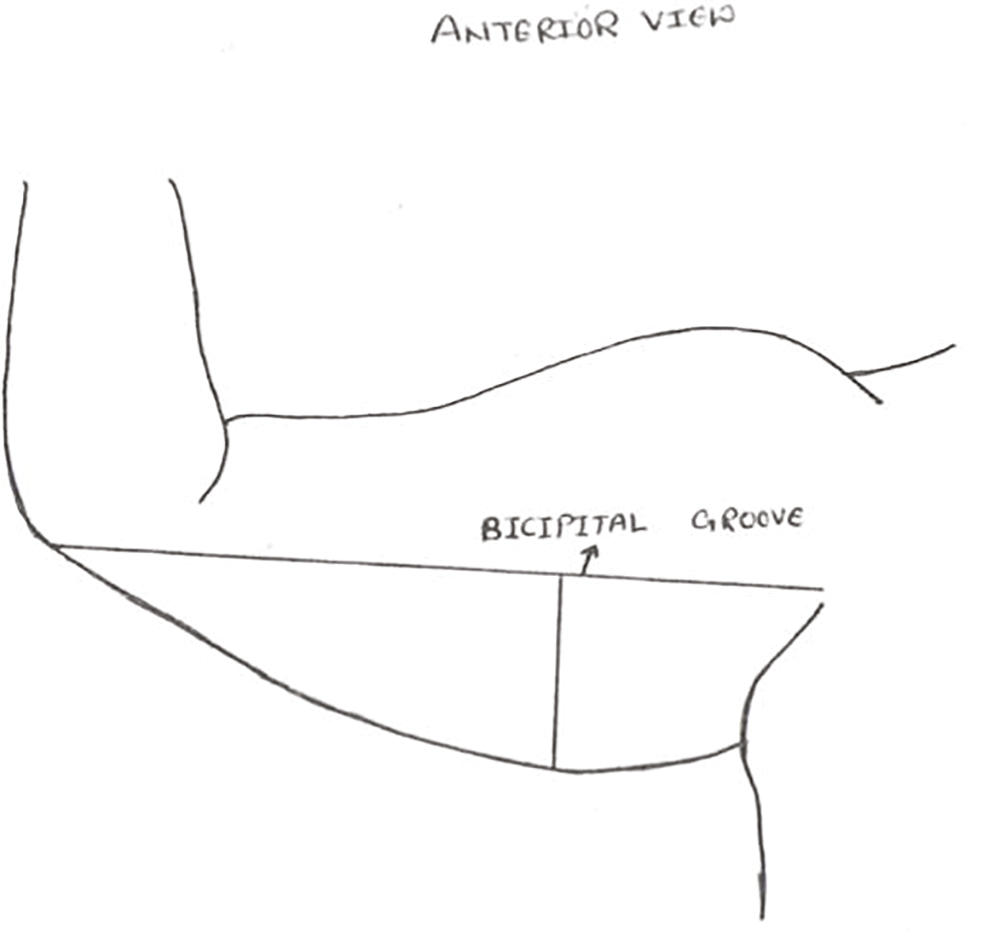
- Bicipital groove imaginary line
The patient was treated with 16 threads per upper arm anteriorly, inferior to the bicipital groove, and 14 threads per upper arm from the posterior approach, inferior to the bicipital groove, as shown in Figures 3 and 4. A total of 30 threads per arm were placed and the same is repeated on day 14.
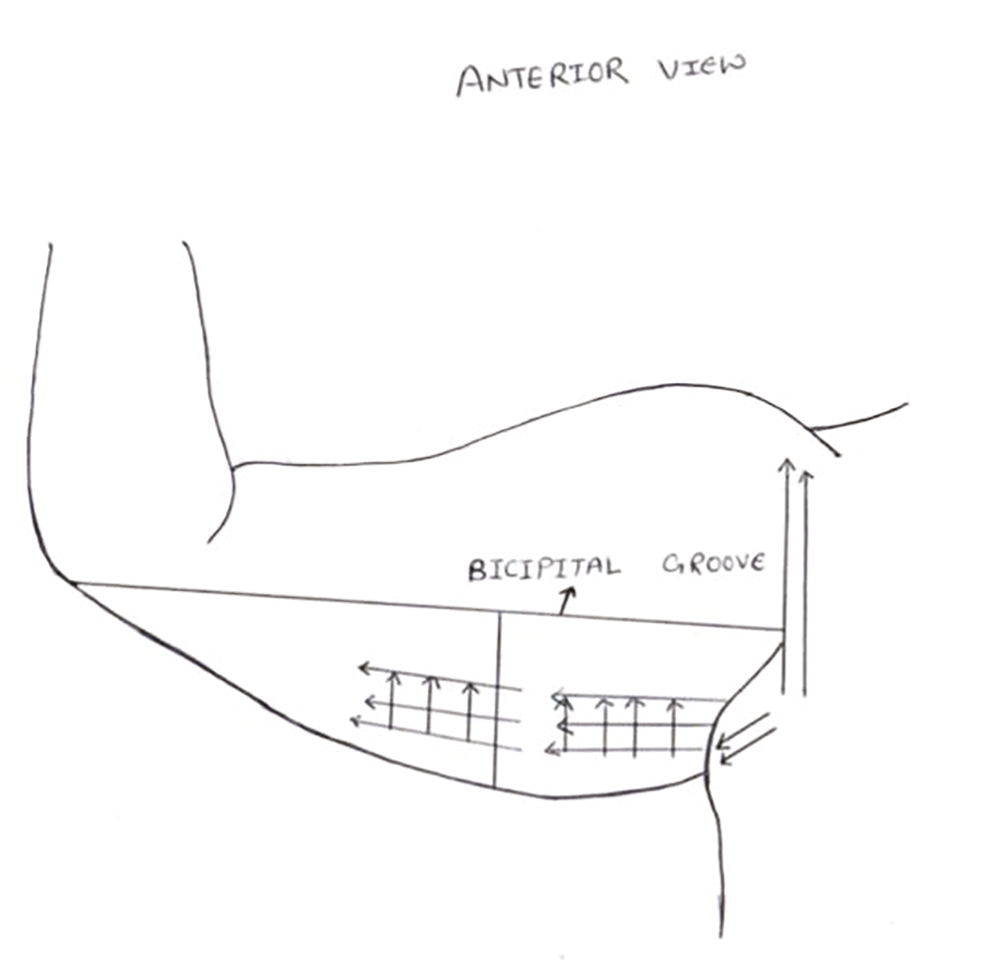
- Anterior view markings for PDO thread placement and the vectors in which placement was done
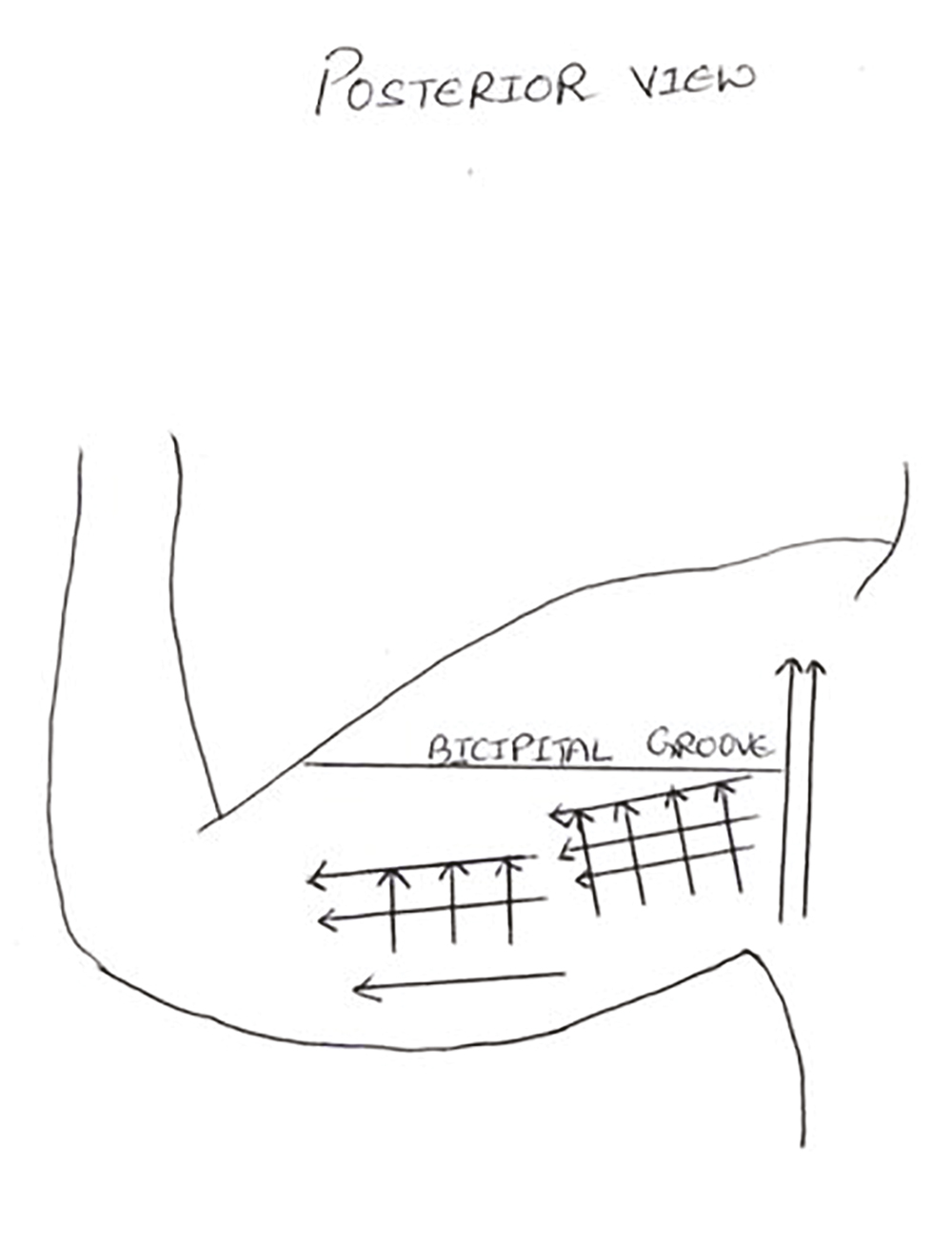
- Posterior view
PDO threads were placed in a mesh pattern working inferior to the line marking of bicipital groove on inferior-medial and inferior-lateral aspects, both anteriorly [Figure 3], and posteriorly [Figure 4]. All threads were placed from deep dermal plane to hypodermis.
Onabotulinum toxin type A was injected on the same day in the inferior-medial, inferior to the bicipital groove of the arm both anteriorly and posteriorly respectively. Each area was treated with 10 U of intradermal onabotulinum A, diluted with 10 mL of preserved normal saline. Therefore, each arm was treated with 20 U of toxin.
Inferior-medial area, inferior to the bicipital groove line, was marked in a mesh pattern making a 10 cm by 2 cm rectangle divided into 20 small squares of 1 cm by 1 cm boxes; the placement is shown in Figures 5 and 6, respectively.
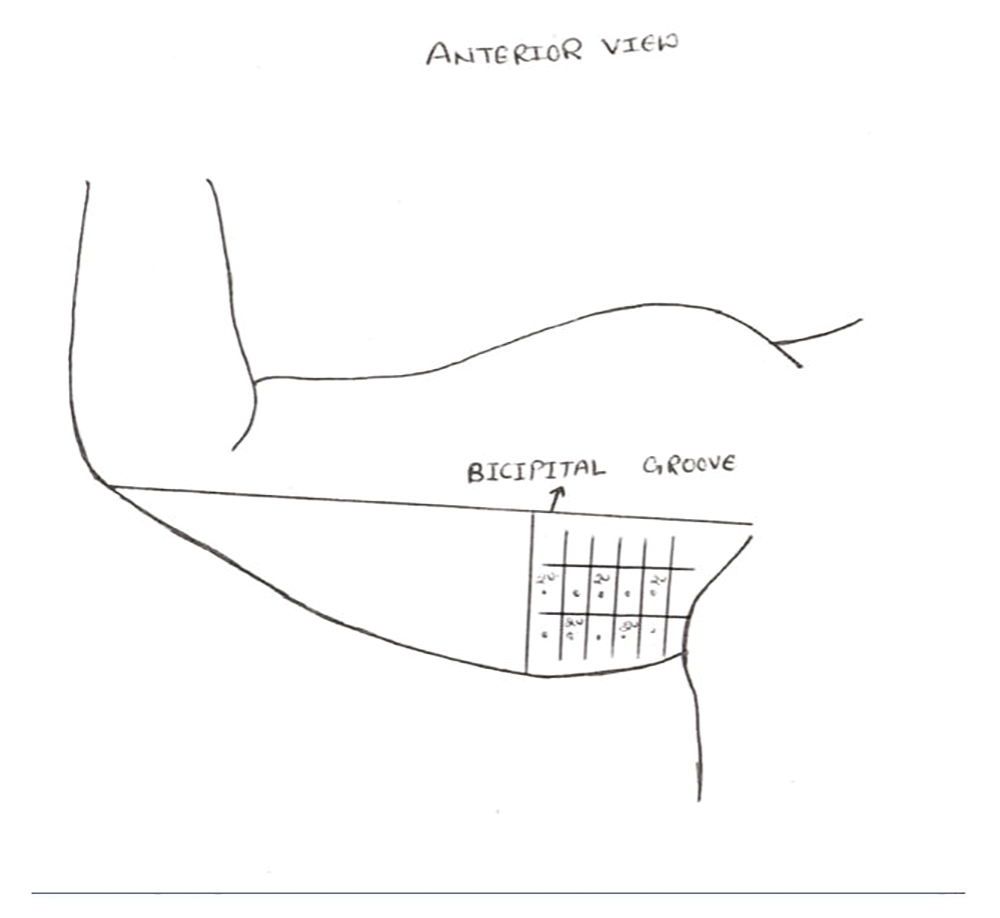
- Markings on anterior aspect arm for injection, and medial half of arm was injected as shown
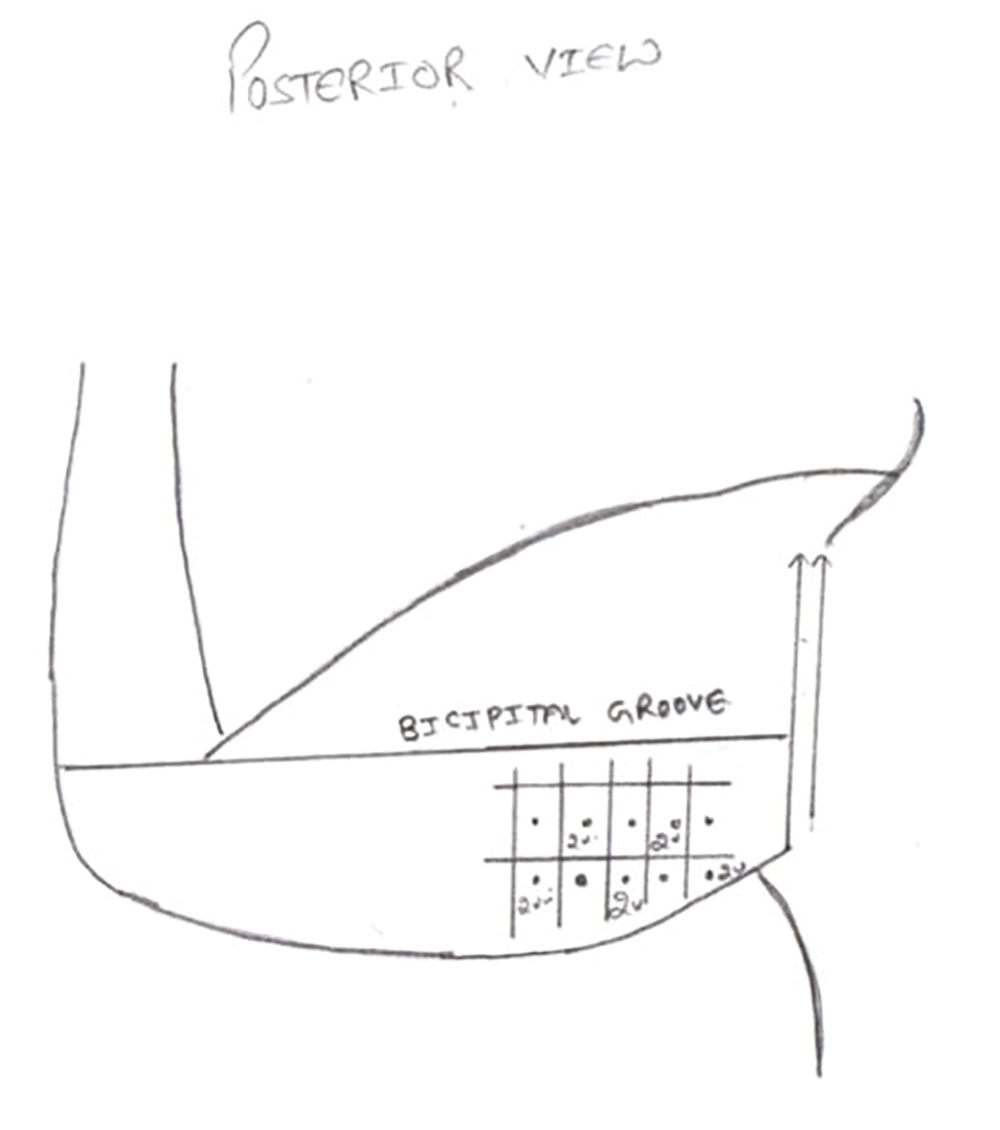
- Markings on posterior aspect of arm for injection
Each grid was injected with 0.5 mL onabotulinum toxin per site. An aliquot of 1 mL/10 U was injected inferio-medially in the anterior aspect and the same was repeated inferio-medially in the posterior aspect.
The area injected showed maximum skin laxity and wrinkles. Improvement was achieved in the laxity observed both by patient and physician on day 30 post-treatment. The patient was photographed on day 0, day 30, and day 90. Results are shown in Figures 7,8–9.

- Clinical photographs of patient on day 0.

- Clinical photographs of patient on day 30.

- Clinical photographs of patient on day 90. Further improvements seen at day 90 after the procedure
DISCUSSION
There are various techniques described to address the clinical condition of skin laxity post-liposuction or weight loss in arm area, the most popular being surgical brachioplexy.[3]
The report focusses on non-surgical options. Existing literature shows evidence of using cryolipolysis, radiofrequency (RF), and focussed ultrasound with some success.[4] RF devices alone or in addition to ultrasound have been used to improve skin laxity with significant results; however, patients need to undergo multiple treatments with a minimum duration of 45 min.[5] Both these technologies generate collagen remodeling and neocollagenesis.[6]
Skin texture and laxity of arm have been addressed by modalities which stimulate collagen to improve the texture and quality of the skin. There is some clinical evidence which shows that PDO threads can stimulate collagen synthesis.[7] The use of PDO threads has been made in facial lifting and reduction of tissue sag with different types of resorbable threads, including PDO.
Intradermal onabotulinum A has been for intradermal injections for facial rejuvenation, showing some improvement in the skin texture.[8] There is some evidence of tightening and improvement in skin appearance after intradermal injections with botulinum toxin A.[9] The improvement in skin texture with intradermal injections of onabotulinum A has been used in this case.
Use of PDO threads in combination with onabotulinum A is a quicker option and requires only two sessions. This may be a suitable technique which may be acceptable to patients as in this case study.
PDO threads are more accurate in placement following vectors with minimal downtime and patient acceptance, making it an elegant and quick approach in combination with onabotulinum A for treatment. The case report gives encouraging suggestions to consider and to further research this technique.
CONCLUSION
PDO threads and onabotulinum A combination for improvement in arm skin laxity following significant voluntary weight loss can give a modest improvement to the patients seeking non-surgical interventions. There is scope to consider a further evaluation of this novel technique.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Rejuvenation of the upper arm. Plast Reconstr Surg. 1998;102:545-51. discussion 552-3
- [Google Scholar]
- Superficial fascial system (SFS) of the trunk and extremities: A new concept. Plast Reconstr Surg. 1991;87:1009-18.
- [Google Scholar]
- Avulsion brachioplasty: Technique overview and 5-year experience. Plast Reconstr Surg. 2014;133:283-8.
- [Google Scholar]
- Treating multiple body parts for skin laxity and fat deposits using a novel focused radiofrequency device with an ultrasound component: Safety and efficacy study. J Cosmet Dermatol. 2017;16:476-9.
- [Google Scholar]
- Rejuvenation of the ageing arm: Multimodal combination therapy for optimal results. Dermatol Surg. 2016;42:S119-23.
- [Google Scholar]
- The efficacy of powdered polydioxanone in terms of collagen production compared with poly-L-lactic acid in a murine model. J Cosmet Dermatol. 2019;18:1893-8.
- [Google Scholar]
- Multiple intradermal small bolus injections of botulinum toxin: The limit and the potentiality. J Cosmet Laser Ther. 2012;14:304-6.
- [Google Scholar]
- Assessment of skin physiology change and safety after intradermal injections with botulinum toxin: A randomized, double-blind, placebo-controlled, split-face pilot study in rosacea patients with facial erythema. Dermatol Surg. 2019;45:1155-62.
- [Google Scholar]




