
Translate this page into:
Novel Method of Treatment of Post-Q-Switched Nd-YAG Laser Depigmentation with Trichloroacetic Acid: A Report of Two Cases
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Q-Switched Nd-YAG laser (SPECTRA: LUTRONIC) has revolutionised the treatment of pigmentary lesions, which otherwise do not respond to medical line of treatment. In spite of its versatile applications, there is often a fear of post-inflammatory depigmentation (PID) especially in Fitzpatrick skin types 3-6. We would like to share our experience of treating two cases of post–Q-switched Nd-YAG laser depigmentation with 65% trichloroacetic acid (TCA) with complete re-pigmentation.
A 27-year-old male patient was started on Q-switched 1064 nm-Nd YAG laser for Nevus of Ota with energy of 6-8.6 J and 3-6 mm spot size. The laser therapy was continued with an interval of 6 weeks between each session. After 15 sessions, the patient developed PID [Figure 1a]. Patient was initially treated with excimer laser for 10-15 sessions with no re-pigmentation. He was then treated with 65% TCA. Degreasing with soap and water was done, all depigmented macules were marked within 1 cm2 area and 65% TCA was applied using toothpick. Frosting was seen in 10-15 s. It was done in five sessions in divided areas. Sunscreen was advised. Complete re-pigmentation was seen in 2-4 weeks [Figure 1b]. The patient is currently under follow up and re-pigmentation is maintained even after 6 months [Figure 1c]. We came across yet another case of post–Nd-YAG depigmentation in a 17-year-old female treated for facial rejuvenation and skin lightening with energy of 1.6-2 J, 8 mm spot size and three passes for 10 sessions. After second session she developed PID [Figure 2a]. She was treated with 65% TCA and the procedure was carried out similarly. Few areas of complete re-pigmentation and crusting were seen in 2 weeks [Figure 2b]. The re-pigmentation is maintained even after 3 months [Figure 2c].
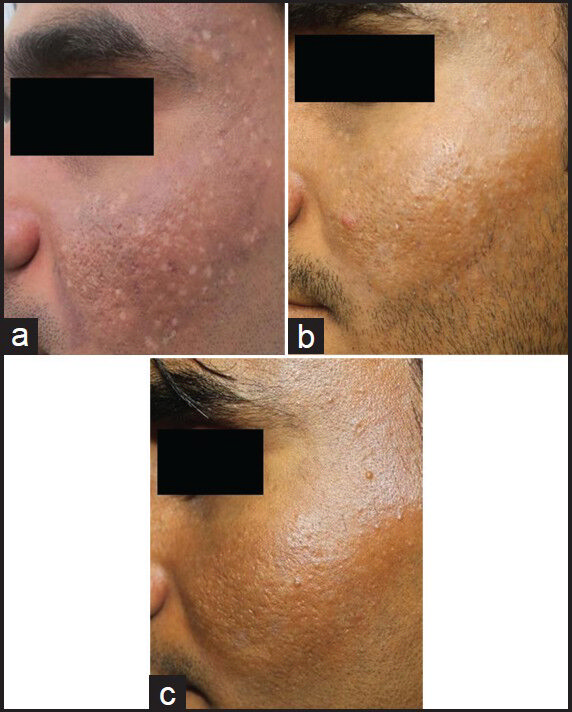
- (a) Patient with Nevus of Ota with mottled depigmentation following 15 sessions of Q-switched Nd YAG laser (b) Complete repigmentation following treatment with 65% trichloroacetic acid after 4 weeks (c) Complete repigmentation persistant at 6 months
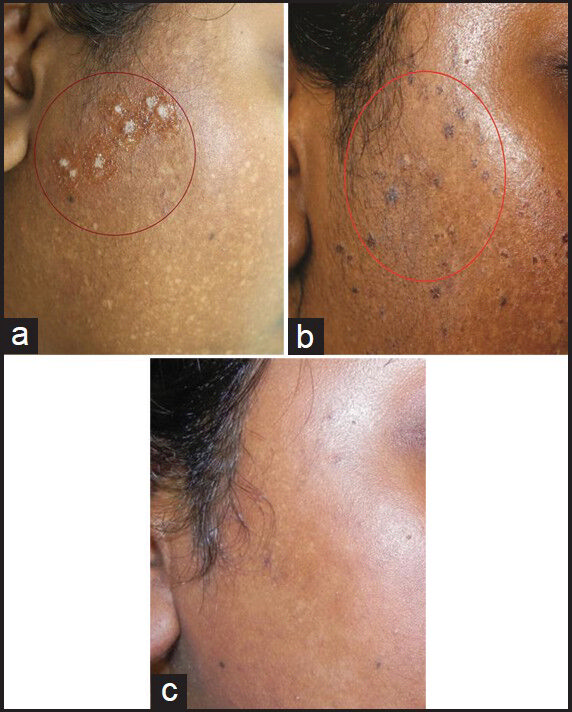
- (a) Patient treated for facial rejuvenation showing mottled depigmenattion following 2 sessions of Q-switched Nd YAG laser (b) Few areas of crusting and complete repigmentation following treatment with 65% trichloroacetic acid after 2 weeks (c) Complete repigmentation persistant at 3 months
While some of the hyperpigmented lesions such as melasma and post-inflammatory hyperpigmentation have no satisfactory medical management; other lesions like Nevus of Ota do not respond to medical management at all. The past decade has developed new systems that are more effective in treating pigmentary lesions such as Q-switched lasers.[1]
Transient complications include immediate erythema, physical urticaria, acneiform eruption, petechiae, whitening of fine hair and rebound hyperpigmentation. Complications, which need stopping the laser therapy, include mottled hypo- and hyperpigmentation, leukoderma, severe urticaria, severe acneiform eruption and herpes simplex activation.[2] It is often stated that PID is difficult to treat and may persist for weeks to months or years. It requires cessation of treatment for a period of 2-3 months, which may be treated with phototherapy.[3] However, the exact incidence of PID as a side effect is not known.
Post-inflammatory hyperpigmentation is a very common complication with TCA in patients with skin type 3-6.[4] We used TCA to treat depigmentation as it is well known to produce side effect of hyperpigmentation. TCA is simple, cost effective and can produce cosmetically acceptable results when complications such as mottled depigmentation are encountered. Hence by these simple techniques of handling the complications, use of Q-switched lasers can be encouraged.
REFERENCES
- Laser for Pigmented lesions and tattoos. In: Mysore Venkatram. In: Textbook on Cutaneous and Aesthetic surgery: Lasers for pigmented lesions and tattoos (1st ed). New Delhi: Jaypee; 2012. p. :799-810.
- [Google Scholar]
- Clinical applications of Q-switched NdYAG laser. Indian J Dermatol Venereol Leprol. 2008;74:682-6.
- [Google Scholar]
- Standard guidelines of care: Lasers for tattoos and pigmented lesions. Indian J Dermatol Venereol Leprol. 2009;75:111-26.
- [Google Scholar]
- Trichloroacetic acid. Step by Step Chemical Peels. (1st ed). New Delhi: Jaypee Medical Publishers; 2009. p. :90-110.
- [Google Scholar]




