
Translate this page into:
Periorbital Rejuvenation: A Study on the Use of Dermal Threads as Monotherapy, with a Review of Literature
Address for correspondence: Dr. Sandeep Arora, Department of Dermatology, Army College of Medical Sciences & Base Hospital, Delhi Cantonment, New Delhi, India. E-mail: aroraderma@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
The periorbital region, a major impressionable area holds a special place in aging of the face. It reflects chronological aging which are reflected not only as structural changes but also emotive expressions of sadness and tiredness. Dermal threads have been used in combination with other aesthetic procedures, however their use as monotherapy especially in periorbital region needs evaluation.
Aim:
To evaluate the improvement in wrinkling and skin texture in the infero-lateral periorbital region with monofilament dermal threads.
Settings and Design:
A prospective observational study in a tertiary hospital was conducted between January 2019 and February 2020 after institutional ethical clearance and patient consent.
Materials and Methods:
25 adults between 40 and 65 years of age reporting for infero-lateral periorbital rejuvenation and opting for dermal threads, with no history of aesthetic treatment in this region for the past three months were included after their informed consent. 10 monofilament dermal threads (5 each in lateral and infraorbital) in either periorbital region were inserted. Cases were assessed with Lemperle’s wrinkle scale and visual analog scale (VAS) and photographic record maintained before procedure and after 16 weeks of procedure. Change in wrinkle grade was analysed using paired t-test and VAS was used to assess patient’s perception of the result.
Results:
25 cases were included in the study, 21 completed the follow-up and 4 were lost to follow up. The mean preprocedure wrinkle score was 2.29 and postprocedure mean scores were 1. This finding was statistically significant. 16 cases were satisfied with their textural improvement (VAS >+2) while 4 reported mild improvement (VAS 2+) and 1 reported no improvement. Side effects observed were bruising in two cases and thread displacement in one case within 24 hours.
Conclusions:
Polydioxanone monothreads offer an alternative aesthetic procedure for periorbital rejuvenation.
Keywords
Periorbital rejuvenation
periorbital wrinkles
polydioxanone thread

INTRODUCTION
The periorbital region holds a special place in aging of the face. It is widely considered as the impressionable region of the face. It is one of the first areas to undergo aging. Aging of this area also reflects the emotional attributes of a person, such as tiredness and sadness. A youthful periorbital region is characterized by a well-defined brow with an appropriate height and a generally pleasant arch defined by gender and personal preferences, smooth and even toned periorbital skin of “good quality,” and a gentle transition to the malar area.[1] Aging, hence, could affect any of these components, resulting in an aged look [Figure 1].
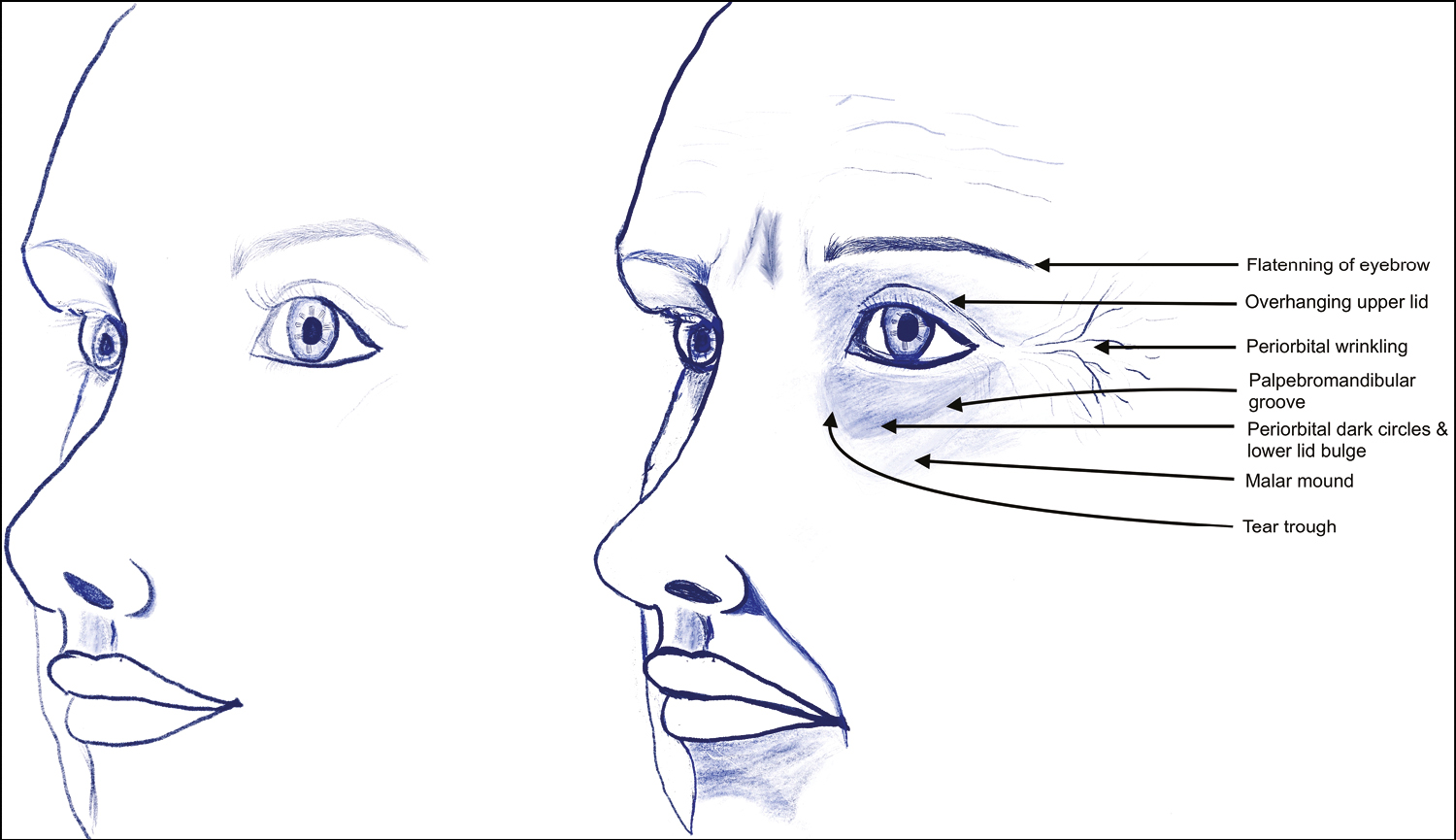
- Profile of periorbital region at younger age (left) and aging changes (right) (original drawing)
Periorbital rejuvenation is, thus, an important component of aesthetic practice and multiple treatment options have been proposed, including surgical correction, hyaluronic acid fillers, botulinum toxin, chemical peels, lasers, mesotherapy, topical preparations, and nutritional supplements alone or in various combinations. Dermal threads have been used for rejuvenation owing to their unique ability to induce collagen remodeling and at the same time induce skin surface changes.[2]
We evaluated 21 cases treated with dermal threads as monotherapy for infero-lateral periorbital rejuvenation to assess their outcomes.
SUBJECTS AND METHODS
Patients between 40 and 65 years of age, reporting to a dermatology center between January 2019 and February 2020 for infero-lateral periorbital rejuvenation and opting for dermal threads treatment, were evaluated after the institute ethical committee clearance and patient consent. Those who had received any other cosmetic procedure for periorbital rejuvenation in the past three months, history of keloidal or bleeding tendencies, pregnant and lactating patients, active infection in this region, unrealistic expectations, and prior allergy to prilocaine/ lidocaine/ material of suture were excluded. All cases were photographed preprocedure and at 16-weeks postprocedure with standard lighting and patient position to ensure uniformity in assessment. They were assessed for periorbital wrinkling severity by using the Lemperle’s scale [Figure 2] (Grade 0: no wrinkles, 1: just perceptible wrinkle, 2: shallow wrinkle, 3: moderately deep wrinkle, 4: deep wrinkle with well-defined edges, and 5: very deep wrinkle with redundant fold),[3] and for the extent of periorbital wrinkling Tamura and Odo classification [Figure 3] was used.[4]
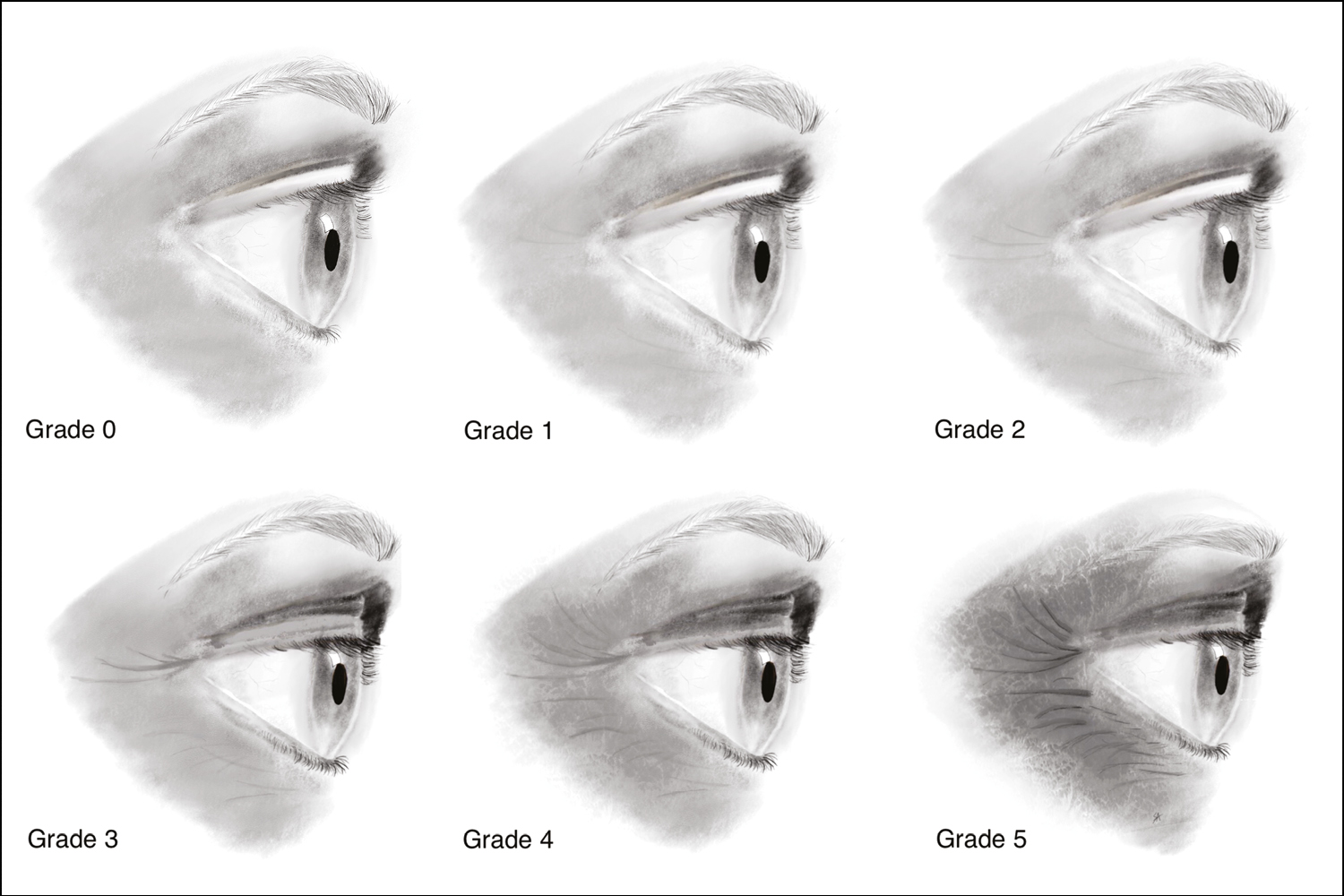
- Lemperle’s wrinkle scale for periorbital region (Grade 0: no wrinkles, 1: just perceptible wrinkle, 2: shallow wrinkle, 3: moderately deep wrinkle, 4: deep wrinkle with well-defined edges, and 5: very deep wrinkle with redundant fold) (original drawing)
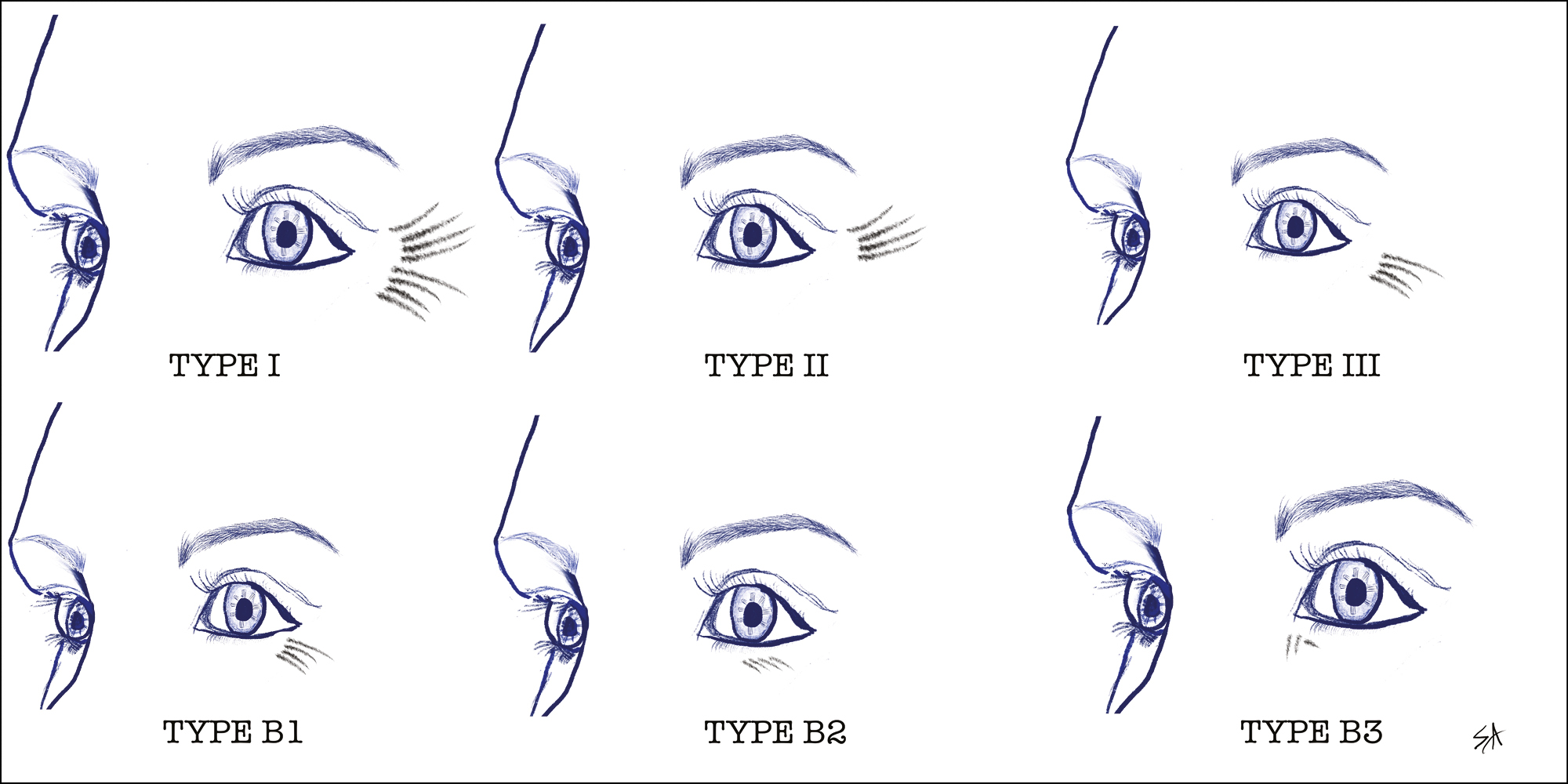
- Tamura and Odo classification of periorbital wrinkles (Type I: lateral periorbital wrinkle extending from the brow to the zygomatic arch; Type II: wrinkles lateral to the external canthus of the eye, extending from the line of the external canthus of the eye to the zygomatic arch with no wrinkles in the superior lateral region; Type III: wrinkles in the line of the external canthus only; presence of lower eyelid wrinkles B1: lateral; B2: medial and B3: internal canthal wrinkles) (original drawing)
Each side was treated with 10 polydioxanone (PDO) monofilament threads (Alfa Aqulift 29G, 25 mm, Yurim Medical, South Korea) in a single session under aseptic precautions with topical anesthesia by using a eutectic mixture of prilocaine and lidocaine 1 h before insertion.
The threads were inserted by using a “pinch and insert method” practised by authors, wherein the skin was pinched at the site of insertion and a needle was inserted. This allowed an easy insertion and enabled the correct plane of delivery. The needles were either inserted singly or more together (depending on the space available to prevent needle crowding) along vectors and removed one after the other with a gentle rotation to ensure thread retention. Five threads were inserted in the infraorbital and five in the lateral periorbital region on either side in the subdermal plane along vectors, as depicted in Figure 4.
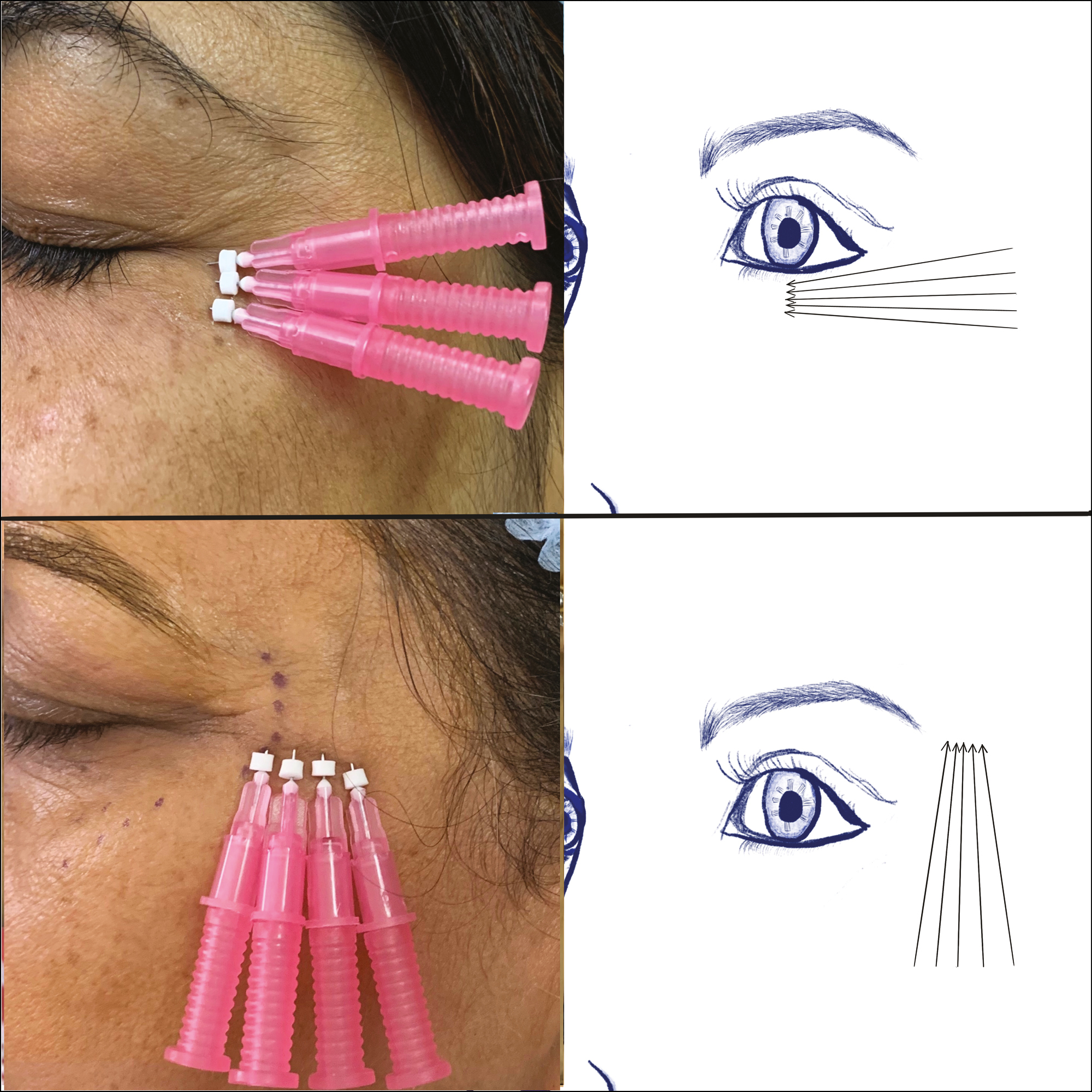
- Representational image of thread insertion in the periorbital region with vectors for infraorbital (above) and lateral periorbital (below) region. (original drawing)
Postprocedure they were advised ice pack application and placed on capsule amoxicillin (625 mg) with clavulanic acid (125 mg) three times a day for five days. Patients were advised to abstain from smoking, vigorous exercises for a week, avoid any face massage for two weeks, and placed on follow-up after one week and every four weeks postprocedure.
The results were assessed by using the score obtained preprocedure and at 16 weeks after the procedure by using the score above and by Visual Assessment Scale (VAS) by patients (4+, >75% improvement; 3+, 50%–75% improvement; 2+, 25%–50% improvement; 1+, 0%–25% improvement; and no response) taking into account textural changes, wrinkle improvement, and skin pigmentation [Figures 5 and 6]. Wrinkle-grade changes were evaluated preprocedure and compared at 16 weeks by using the paired t-test to assess for statistical significance, and VAS was recorded to assess patient satisfaction.
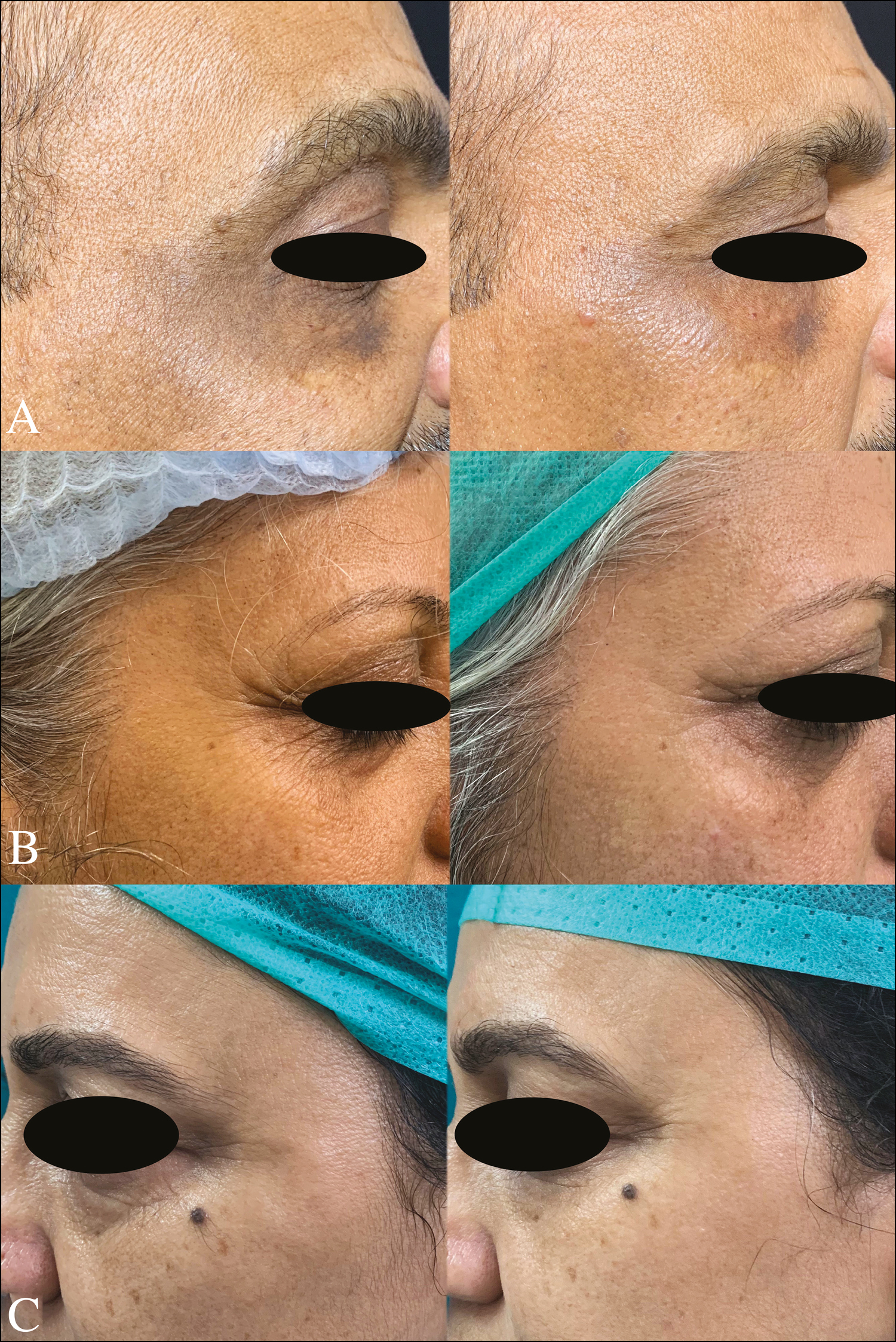
- Preprocedure (left) and postprocedure (right) A: improvement in wrinkles and periocular pigmentation; B and C: improvement in wrinkles and periocular rejuvenation
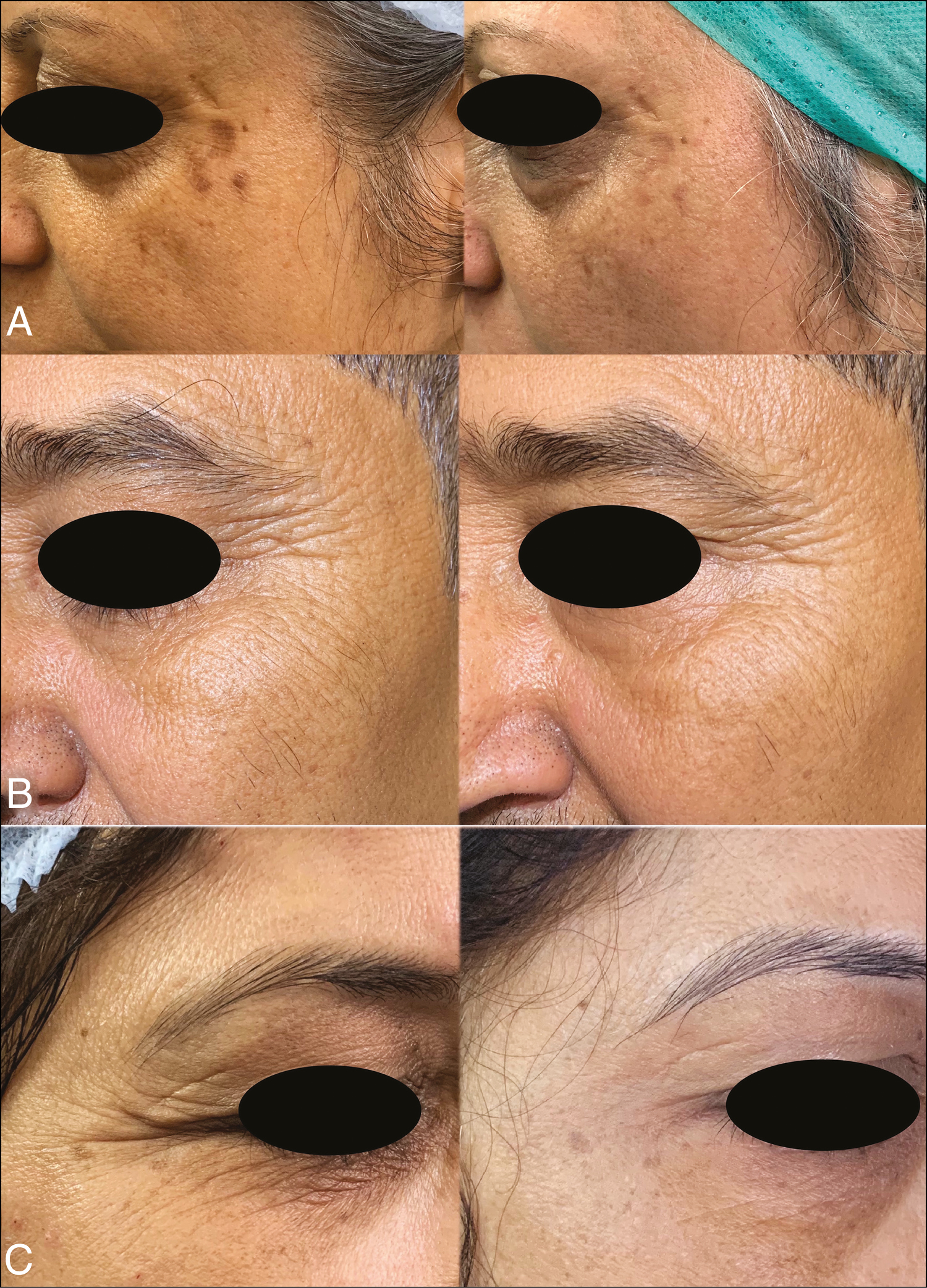
- Preprocedure (left) and postprocedure (right) A: improvement in scar and wrinkles; B: poor response to treatment; C: improvement in wrinkles and rejuvenation
RESULTS
Overall, 25 patients were evaluated and initiated in the study between January 2019 and February 2020. However, 21 (19 females and two males) could be followed up. At the end of 16 weeks, four cases were lost to follow-up, one each after two and three weeks and two after eight weeks. All patients were between 40 and 65 years of age. All cases reported for improvement in skin texture, periorbital wrinkling and three cases also desired improvement of “under eye bags.” The mean preprocedure wrinkle score was 2.29, and postprocedure mean score was 1. The finding was statistically significant (P < 0.0001).
Overall, 16 cases were satisfied with their textural improvement (VAS >+2), four reported mild improvement (VAS 2+), and one reported no improvement [Table 1].
| Serial number | Age (years) | Gender | Signs of aging | Wrinkle pattern | WG pretreatment | WG posttreatment | VAS |
|---|---|---|---|---|---|---|---|
| 1 | 52 | F | W, TC | II B2 | 4 | 1 | 4+ |
| 2 | 47 | F | W, TC, EB | II B1 | 2 | 1 | 3+ |
| 3 | 47 | F | W, TC | I | 1 | 0 | 4+ |
| 4 | 52 | M | W, TC | I B1 | 5 | 3 | 2+ |
| 5 | 53 | M | W, TC | II B2 | 4 | 1 | 4+ |
| 6 | 48 | F | W, TC | II B2 | 2 | 1 | 3+ |
| 7 | 54 | F | W, TC, EB | II B1,B2 | 2 | 1 | 3+ |
| 8 | 48 | F | W, TC | II B1 | 2 | 1 | 2+ |
| 9 | 51 | F | W, TC | II B1,B2,B3 | 3 | 2 | 3+ |
| 10 | 44 | F | W, TC | I B2 | 1 | 0 | 4+ |
| 11 | 41 | F | W, TC | I B1 | 1 | 0 | 4+ |
| 12 | 54 | F | W, TC | II B1 | 2 | 1 | 3+ |
| 13 | 50 | F | W, TC | II B2 | 1 | 0 | 3+ |
| 14 | 57 | F | W, TC | II B1,B2,B3 | 3 | 2 | 2+ |
| 15 | 64 | F | W, TC, EB | II B1,B2,B3 | 4 | 3 | 1+ |
| 16 | 48 | F | W, TC | I | 1 | 0 | 3+ |
| 17 | 44 | F | W, TC | I | 1 | 0 | 4+ |
| 18 | 53 | F | W, TC | II B1,B2 | 2 | 1 | 3+ |
| 19 | 48 | F | W, TC | II B1 | 2 | 1 | 4+ |
| 20 | 52 | F | W, TC | II B1 | 3 | 1 | 3+ |
| 21 | 58 | F | W, TC | II B1,B2 | 2 | 1 | 2+ |
W = wrinkling; TC = textural changes; EB = eye bags; M = male; F = female; WG = wrinkle grade; VAS = Visual Analog Scale
Erythema and periorbital puffiness as sequelae were seen in four cases. Side effects observed were bruising in two cases, which resolved over the next seven days, thread displacement in one case within 24 h after inadvertent rubbing of the periorbital region [Figure 7]. The thread was removed, and an additional thread was placed in the infraorbital region.
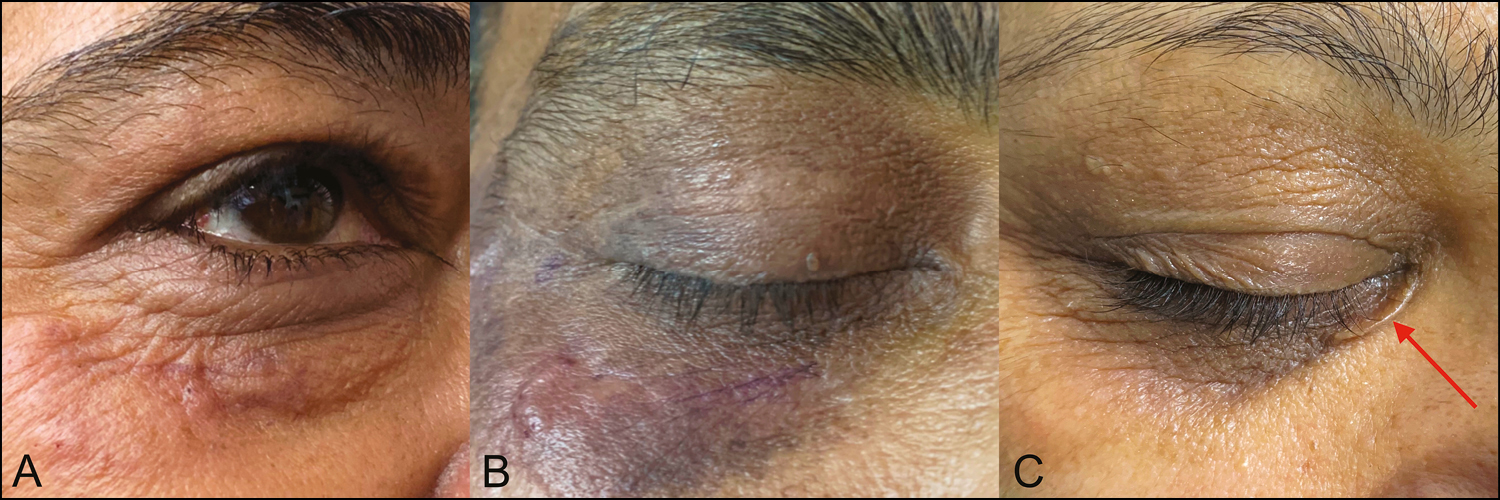
- Sequelae and complications: A: early erythema and edema; B: early linear ecchymosis along thread insertion; C: displaced thread (red arrow)
DISCUSSION
The periorbital region is the presenting region of the face. The complex process of facial aging is best represented in this region. From the underlying bony structure to the various layers of the soft tissue, aging occurs at all anatomical levels. The anatomical understanding of this region is, hence, a must to understand its aging process.
The thin eyelid skin does not contain subcutaneous fat, is less than 1 mm thick, and transitions to the skin of the periorbital region, the brow region superiorly, and the malar area inferiorly. This region has three main fat pads superiorly, the preseptal lying over the orbital septum, the preaponeurotic behind the orbital septum and over the levator aponeurosis, and the galeal located under the brow skin. Inferiorly the three fat pads, medial, central, and lateral lie over the capsulopaplebral fascia and under the orbital septum [Figure 8]. A thin fibrous septum arising from the periosteum of the orbit forms the orbital septum in the inferior and superior region lying below the sphincteric muscle of the eye; the orbicularis oculi, which, in turn, consists of its pretarsal, preseptal, and orbital parts [Figure 8].[1567]
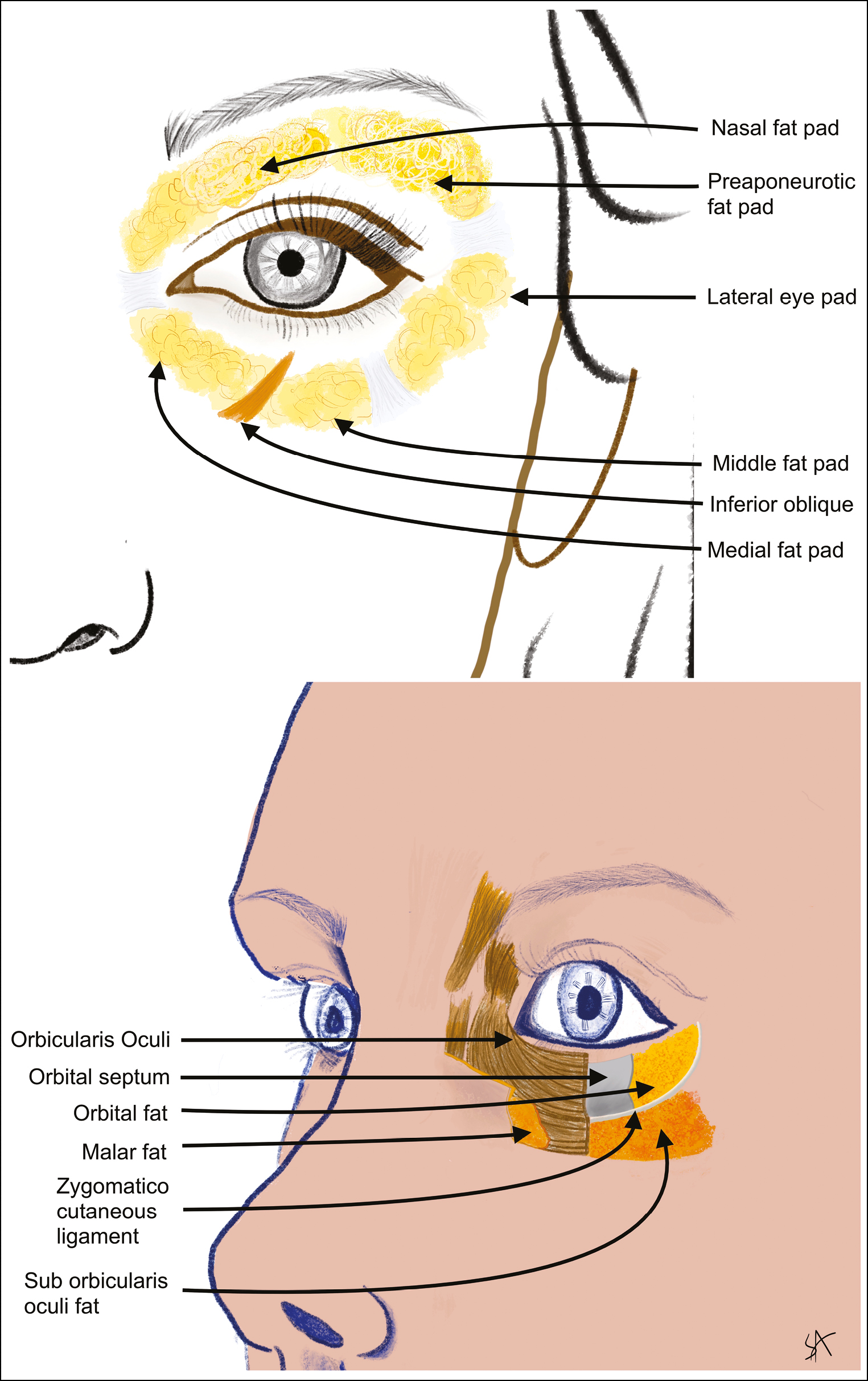
- Periorbital fat pads (above) and transverse section through layers of periorbital region (below) (original drawing)
Aging results in resorption of the bone, fat atrophy, and ligamental and muscular laxity with a shift of action from levators to depressors. The skin is affected by this chronological aging, resulting in a loss of elasticity and hydration as well as the exposome, which cause photoaging and a gravity-dependent tissue sag.[89]
For aging changes and its assessment, the periorbital region is divided into three parts [Figure 9].[6] In zone 1, with age, the eyebrows turn flatter in shape and depress in height appearing to lie at or below the prominent supraorbital rims due to resorption of periorbital frontal and zygomatic bones, fat atrophy, hyperactivity of its depressors as compared with younger brows with their gentle curved arch in females and flatter but higher brows in males; zone 2 changes are the most striking. Baggy lower eyelids have a complex etiopathogenesis. Skin laxity of the lower lid resulting from elastin and collagen degeneration, fluid retention, fat compartment sag by weakening orbicularis muscle, and orbital septum with retroorbital and infraorbital fat pseudo-herniation and orbital resorption result in puffy under eyes. In addition to what has been cited earlier, thinning of the skin with increased visibility of the underlying vascular network and orbicularis oculi, excessive dermal melanogenesis of multifactorial etiology such as melasma, dermal melanocytosis, hemosiderin deposition, and orbital hollowing leading to infraorbital shadowing all result in infraorbital dark circles.[1011] Ligamental tethering along with infraorbital fat sag heightens the transition medial eyelid to the maxilla, forming the tear trough and from the lateral lower eyelid to the zygoma forming the palpebro-malar groove [Figure 1].[7] Zone 3 merges with the midface.
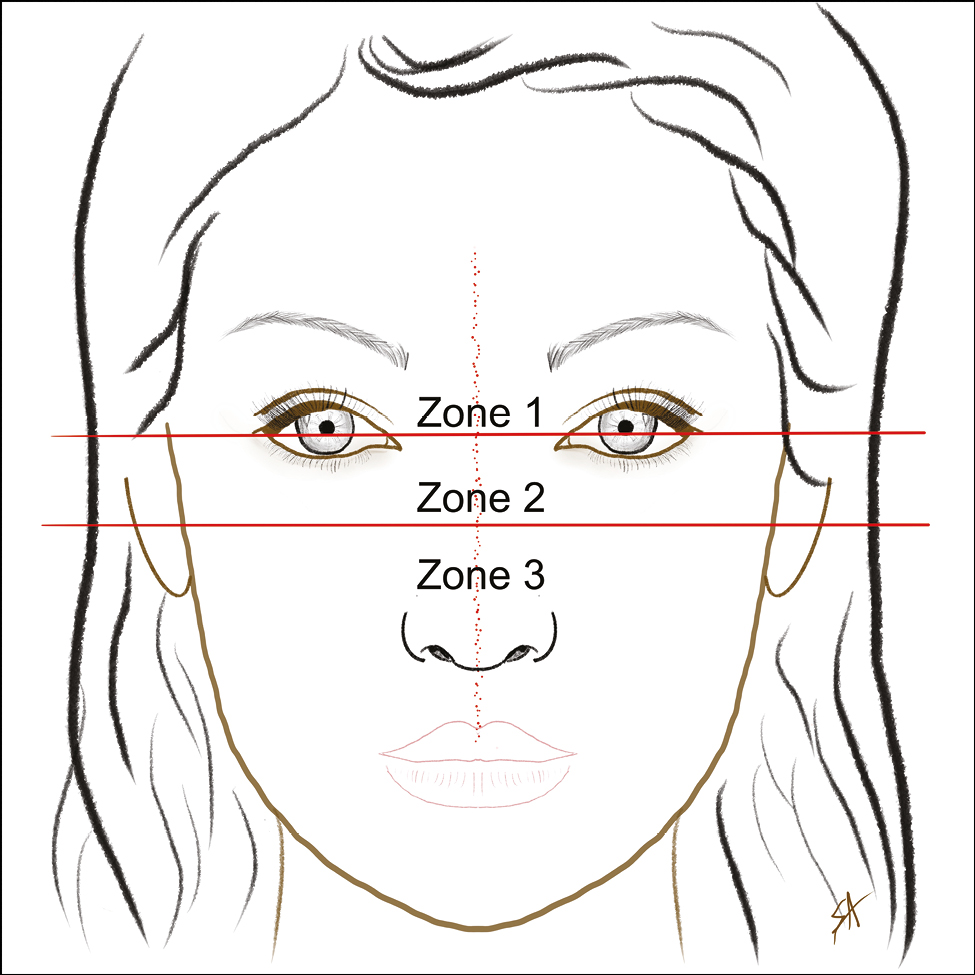
- Periorbital zones (original drawing)
Nonsurgical treatments for periorbital rejuvenation include topical therapies in the form of sunscreens, retinoids, peptides, antioxidants, chemical peels, laser and mechanical resurfacing, botulinum toxin, nonablative and microneedle radio frequency devices and dermal fillers, boosters, carboxytherapy, and platelet-rich plasma.[121314151617181920] Dermal threads are increasingly being used for lift and rejuvenation, especially on the face, as they stimulate fibroblasts, induce collagenization, and neo-angiogenesis, thus improving the skin texture, laxity, and wrinkles.[221,22] They can, thus, be used in areas that are classically the no-go areas for other procedures such as the infraorbital for botulinum toxin in infraorbital wrinkling. To the best of our knowledge, there is no reported literature on these.
One type of monofilament threads was used in all our cases, hence ensuring uniform assessment of results and clinical outcome.[23] Literature reports are varied, especially for anchored or barbed threads as the final outcome would be dependant in these cases on the thread’s tensile strength, surgeon techniques, and vectors used. The PDO threads induce tissue changes and are generally free from these mechanical variables.[24]
In our cases, those with mild to moderate wrinkling and textural changes reported higher degree of satisfaction (VAS > 2+), however those with severe wrinkling, and “under eye bags” reported lower satisfaction and were also observed to have responded poorly to the procedure [Figures 5 and 6]. The complex multifactorial etiology of under eye puffiness emphasizes that no one single procedure may benefit these cases and each individual must be assessed and treated accordingly. Improvement in skin color with improvement in “dark circles” could possibly be explained by collagen induction and the subsequent increase in skin thickness, resulting in altered optical properties of the erstwhile thinner skin here.
Side effects reported after monothreads insertion are usually edema, swelling, and pain.[2526] Four of our cases had erythema and transient swelling, which lasted a few hours to the next 24 h and those subsided without intervention. Two of our cases had bruising, which subsided over the next 10 days. They were advised topical vitamin K cream twice a day for seven days. The periorbital area is vascular rich and especially at risk of postoperative ecchymoses and hematomas. Thinner 29-gauge needles used in the procedure possibly prevented a more common occurrence of this complication. One patient had inadvertently rubbed her eye a few hours after the procedure, resulting in the displacement of a single thread that was removed the next day by a needle stab incision. Hence, there was a need for care of the treated area for a week postprocedure to prevent thread displacement. Since the threads were placed subdermally, their migration to deeper layers beyond this plane was not possible and were, hence, considered safe. Frequent inadvertent blinking on account of the active orbicularis oculi or inadvertent rubbing, as in our case, may cause thread migration in the same plane. This, nevertheless, emphasizes the need for a trained dermatologist/ aesthetic physician to practice this procedure to ensure the correct delivery of the thread.
Our study was limited by a smaller size, and larger studies may be needed to corroborate the results.
CONCLUSION
The PDO threads offer an important additional approach to rejuvenation, especially in the periorbital region, with minimal adverse effects encountered in other aesthetic procedures and surgery.[2728] They may be combined with other modalities such as botulinum toxin, dermal fillers, and skin boosters to further enhance their rejuvenating potential. As with other aesthetic procedures, repeated sessions may be needed to maintain their effect. Those with severe wrinkling may benefit with repeated sessions. The use of longer lasting materials such as polycaprolactone and microlifting using PDO threads with exosomes could enhance the effectiveness of this procedure.[2930]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/ have given his/ her/ their consent for his/ her/ their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Continuing medical education examination—facial aesthetic surgery in pursuit of optimal periorbital rejuvenation: Laser resurfacing with or without blepharoplasty and brow lift. Aesthet Surg J. 1998;18:321-32.
- [Google Scholar]
- A classification of facial wrinkles. Plast Reconstr Surg. 2001;108:1735-50; discussion 1751-2.
- [Google Scholar]
- Classification of periorbital wrinkles and treat- ment with Botulinum Toxin Type A. Surg Cosmet Dermato. 2011;3:129-34.
- [Google Scholar]
- New medical approach for rejuvenation of the periorbital area. Clin Med Investig. 2016;1:27-30.
- [Google Scholar]
- Periorbital facial rejuvenation; applied anatomy and pre-operative assessment. J Curr Ophthalmol. 2017;29:154-68.
- [Google Scholar]
- Study on the aging dynamics of the periorbital region: From observation to knowledge of physiopathology. Ophthal Plast Reconstr Surg. 2019;35:333-41.
- [Google Scholar]
- The role of gravity in periorbital and midfacial aging. Aesthet Surg J. 2014;34:809-22.
- [Google Scholar]
- Infraorbital dark circles: A review of the pathogenesis, evaluation and treatment. J Cutan Aesthetic Surg. 2016;9:65.
- [Google Scholar]
- Clinical analysis and classification of dark eye circle. Int J Dermatol. 2014;53:164-70.
- [Google Scholar]
- Periorbital rejuvenation: A review of dermatologic treatments. Dermatol Surg. 1999;25:1-9.
- [Google Scholar]
- Periorbital hyperpigmentation: A comprehensive review. J Clin Aesthet Dermatol. 2016;9:49-55.
- [Google Scholar]
- Periorbital chemical peels. In: Myint SA, ed. Nonsurgical Peri-orbital Rejuvenation. Boston, MA: Springer US; 2014. p. :25-38. Available from: http://link.springer.com/10.1007/978-1-4614-8388-5_3 [cited 2020 Oct 16]
- [Google Scholar]
- Treatment of periorbital dark circles: Comparative study of carboxy therapy vs chemical peeling vs mesotherapy. J Cosmet Dermatol. 2019;18:169-75.
- [Google Scholar]
- Hyaluronic acid filler for skin booster on the face. In: Issa MCA, Tamura B, eds. Daily Routine in Cosmetic Dermatology. Cham: Springer International Publishing; 2017. p. :1-10. Clinical Approaches and Procedures in Cosmetic Dermatology. Available from: http://link.springer.com/10.1007/978-3-319-20253-2_23-1 [cited 2020 Oct 16]
- [Google Scholar]
- Resurfacing with ablation of periorbital skin technique: Indications, efficacy, safety, and 3D assessment from a pilot study. Photomed Laser Surg. 2018;36:541-7.
- [Google Scholar]
- Microneedling: Advances and widening horizons. Indian Dermatol Online J. 2016;7:244.
- [Google Scholar]
- Update in minimally invasive periorbital rejuvenation with a focus on platelet-rich plasma: A narrative review. J Cosmet Dermatol. 2020;19:1057-62.
- [Google Scholar]
- Platelet Rich Plasma – where do we stand today? A critical narrative review and analysis. Dermatol Ther. [cited 2020 Sep 30]; Available from: https://onlinelibrary.wiley.com/doi/10.1111/dth.14343
- [Google Scholar]
- Thread-lift for facial rejuvenation: assessment of long-term results. Arch Facial Plast Surg. 2009;11 Available from: http://archfaci.jamanetwork.com/article.aspx?doi=10.1001/archfacial.2009.10 [cited 2019 Dec 7];
- [Google Scholar]
- Polydioxanone threads for facial rejuvenation: Analysis of quality variation in the market. Plast Reconstr Surg. 2019;144:1002e-9e.
- [Google Scholar]
- Thread-lift sutures: Still in the lift? A systematic review of the literature. Plast Reconstr Surg. 2018;141:341e-7e.
- [Google Scholar]
- A study of complications of aesthetic thread lift: A review of 250 cases. Available from: http://rgdoi.net/10.13140/RG.2.2.32103.88489
- [Google Scholar]
- Noncosmetic periocular therapeutic applications of botulinum toxin. Middle East Afr J Ophthalmol. 2010;17:113.
- [Google Scholar]
- Complications of hyaluronic acid fillers and their managements. J Dermatol Dermatol Surg. 2016;20:100-6.
- [Google Scholar]
- Micro-shuttle lifting of the neck: A percutaneous loop suspension method using a novel double-ended needle. Aesthet Surg J. 2016;36:629-38.
- [Google Scholar]
- Combining PDO threads with exosomes for microlifting. Cosmetic Surgery [Internet]. IntechOpen; 2021 [cited 2020 Oct 19] https://www.intechopen.com/books/cosmetic-surgery/combining-pdo-threads-with-exosomes-for-microlifting
- [Google Scholar]




