
Translate this page into:
Platelet-rich fibrin therapy as an adjuvant treatment in the management of metastatic Crohn’s disease: A case series
*Corresponding author: Shekhar Neema, Department of Dermatology, Armed Forces Medical College, Pune 411040, Maharashtra, India. shekharadvait@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vasudevan B, Neema S, Vendhan S. Platelet-rich fibrin therapy as an adjuvant treatment in the management of metastatic Crohn’s disease: A case series. J Cutan Aesthet Surg. 2025;18:138-40. doi: 10.4103/JCAS.JCAS_59_23
Abstract
Metastatic or cutaneous Crohn’s disease (MCD) is a rare manifestation of Crohn’s disease and presents with ulcers, nodules, edema, fissures, and fistula. The genital involvement is seen in almost 50% patients and linear ulcers (knife-cut ulcers) are characteristic clinical features. The histopathological findings of skin lesions are similar to gastrointestinal involvement and are diagnostic. The treatment options for the management of MCD include topical and oral steroids, oral metronidazole, as well as immunosuppressants such as methotrexate, azathioprine, cyclosporine, and tumor necrosis factor alpha inhibitors. We present three cases of MCD who were treated with platelet-rich fibrin therapy as adjuvant and resulted in rapid healing of ulcers.
Keywords
Crohn’s disease
Cutaneous Crohn’s disease
Platelet-rich fibrin
Platelet-rich metastatic Crohn’s disease
PRF
PRP
Therapy
Treatment

INTRODUCTION
Cutaneous symptoms are seen in 22%–44% of Crohn’s disease (CD) patients at some point during the course of their illness.1 Inflammatory bowel disease-related cutaneous lesions have been classified as: Specific lesions (same histopathologic features as the underlying gastrointestinal disease), reactive lesions (inflammatory process; does not share the gastrointestinal pathology), and associated diseases (human leukocyte antigen linkage phenotype and sequelae of chronic inflammation).2 Metastatic Crohn’s disease (MCD) also known as cutaneous CD and is defined by granulomatous skin lesion discontinuous from the affected gastrointestinal tract. It presents with nodules, ulcerations, crusts, erosions, erythematous, and violaceous plaques and perianal and peristomal fissures and fistula. The cutaneous linear erosions seen in MCD are referred to as “knife-cut” ulcers. Almost 50% adults with MCD have genital involvement that presents as ulceration, erythema, edema involving scrotum, penis, vulva, labia, and perineum. It can develop before, alongside, or after gastrointestinal symptoms.3
We hereby report a case series of three patients with cutaneous CD successfully managed with platelet-rich fibrin (PRF) therapy as an adjuvant treatment.
The first case was a 30-years-old male patient, a known case of CD, presented with multiple linear ulcers in inguinal folds, scrotum, and penis of two years duration. He was thin-built and malnourished. Histopathology was consistent with CD and skin swab was negative for infections [Figure 1]. For gastrointestinal symptoms, he was treated with azathioprine 100 mg in divided doses and infliximab @5 mg/kg every 8 weeks, that led to improvement in his gastrointestinal symptoms without much improvement in skin condition even after 6 months. He was given weekly PRF treatment [Figure 2] and showed significant improvement in ulcers after 4 weeks [Figure 3a and b].
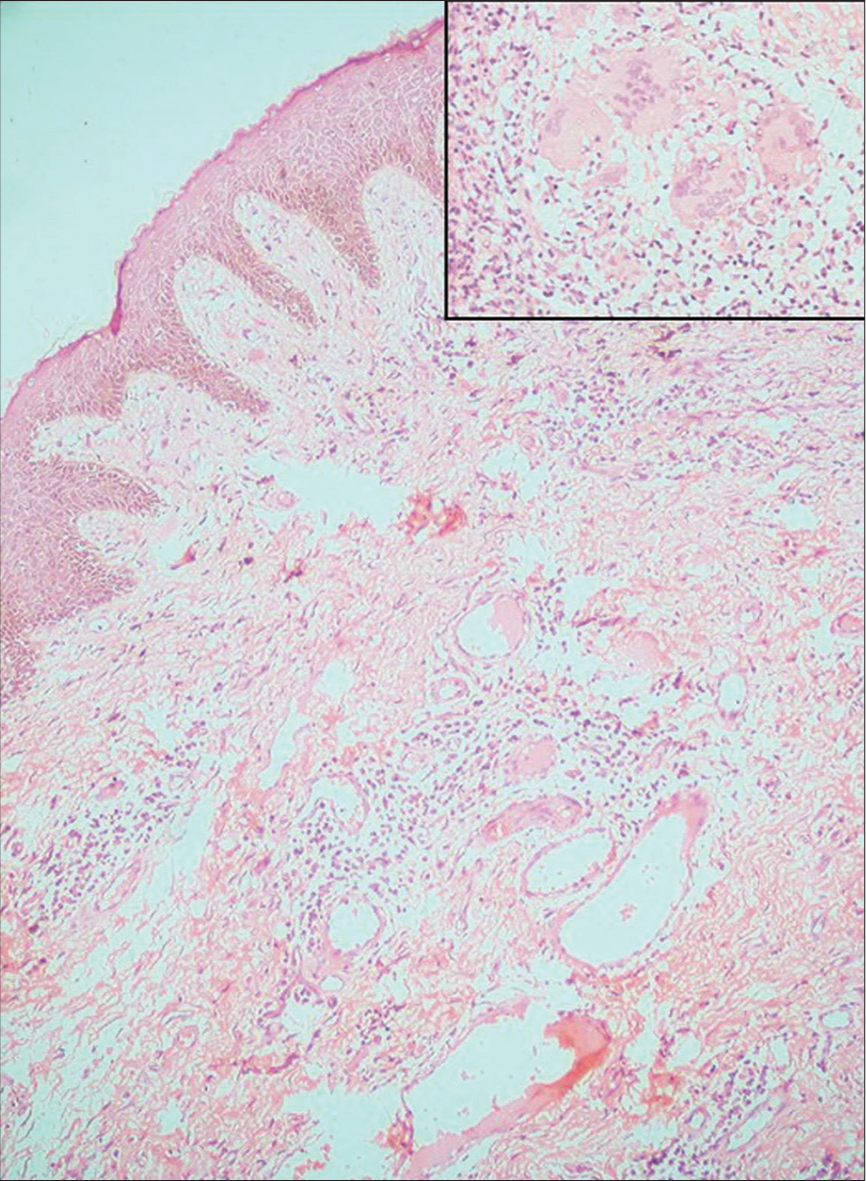
- Histopathological examination from the lesion showing Langerhans giant cells and epithelioid granulomas suggestive of Crohn’s disease (H&E, 400×) Inset – 1000×. H&E: Hematoxylin and eosin.
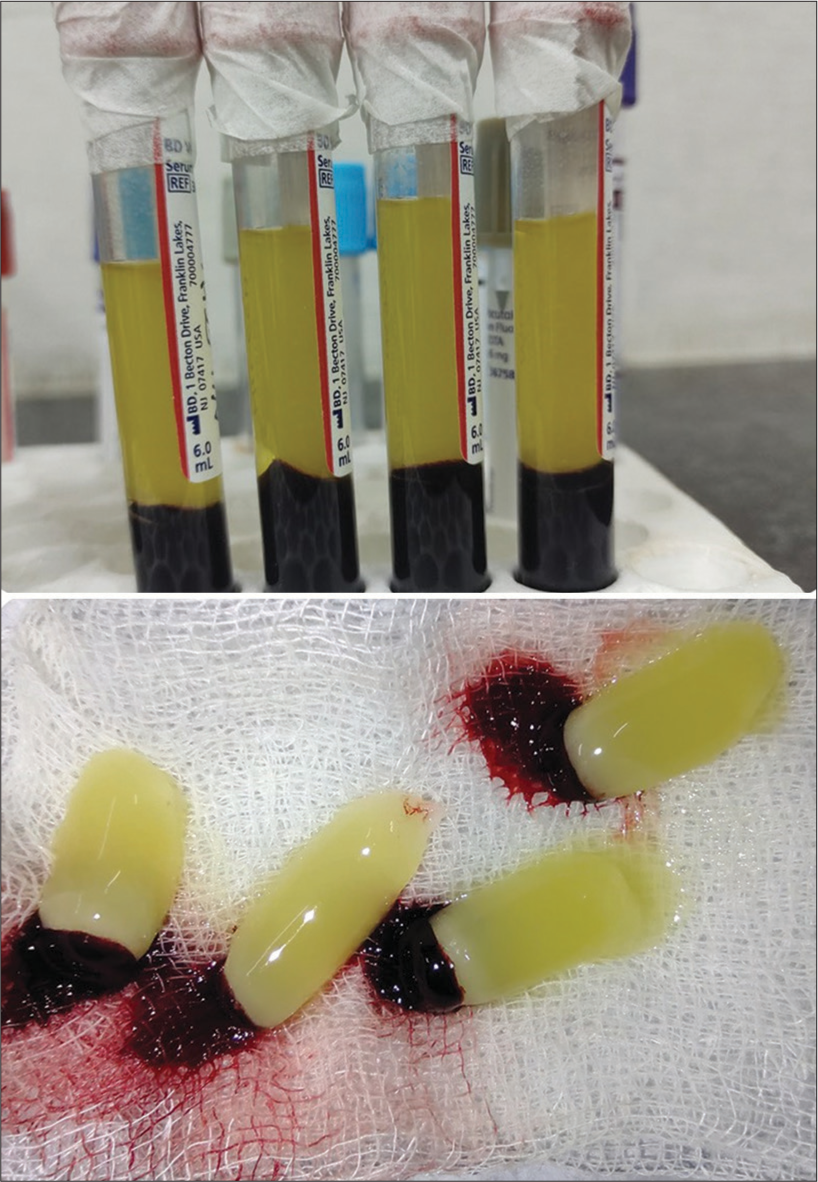
- Platelet-rich fibrin with red blood cell (RBC) tail. This platelet-rich fibrin (PRF) is placed on the wound and dressing is done.

- (a) Knife-cut ulcer in groin fold. (b) Complete healing of ulcer after weekly sessions of platelet-rich fibrin (PRF) after 4 weeks. (c) Knife-cut ulcer in suprapubic region. (d) Complete healing seen after weekly PRF after 3 weeks.
The second case was a 33-years-old female patient, with no bowel symptoms, presented with multiple linear ulcers in inguinal folds, perianal area, and lower abdomen of 8 years duration. Histopathology of ulcers were consistent with CD, however, colonoscopy, contrast enhanced computerized tomography abdomen and anti- Saccharomyces cerevisiae antibodies were within normal limits. The patient was treated with prednisolone 30 mg per day along with azathioprine @ 2 mg/kg/day with partial response at 12 weeks; weekly PRF treatment for ulcers was started and ulcer healed completely at 3 weeks [Figure 3c and d].
The third case was a 31-year-old male patient, presented with a linear ulcer over the intergluteal region and shaft of penis for the last 6 months. Skin biopsy was suggestive of CD; however, there was no other evidence of CD. The patient was started on prednisolone 30 mg/day along with weekly platelet-rich fibrin dressing and resulted in significant improvement at 3 weeks.
DISCUSSION
MCD is a rare disease and generally occurs in patients with established gastrointestinal disease, however, it may precede gastrointestinal involvement by months to years. The histopathology of involved skin shows non-caseating granulomas and histiocytes similar to gastrointestinal tract involvement.3
The treatment of MCD depends on the severity of the involvement and single lesions can be treated with topical or intralesional corticosteroids. Systemic treatment options include oral glucocorticoids, oral metronidazole, immunosuppressant such as methotrexate, cyclosporine, azathioprine, and tumor necrosis factor-α inhibitors such as adalimumab and infliximab. Hyperbaric oxygen has also been tried in the management.4 Platelet-rich plasma (PRP) is an autologous blood product and PRP injections have been used for the management of fistula and were found to be effective.5 PRP releases many growth factors and helps in wound healing. PRF is a second-generation autologous blood product. It is simpler to prepare, does not require anticoagulants, and does not need to be injected as PRP. Unlike PRP, it releases growth factors slowly and acts as scaffolding for better wound healing.6,7 To the best of our knowledge, PRF has not been used earlier for the management of MCD. It is a safe and effective adjuvant in the treatment of this difficult disease.
Authors’ contributions
All the authors contributed to the research study. Biju Vasudevan: Concepts, Design, Definition of intellectual content, Literature search, Manuscript preparation, Manuscript Editing, and Manuscript review. Shekhar Neema: Concepts, Design, Definition of intellectual content, Literature search, Manuscript preparation, Manuscript Editing, and Manuscript review. Senkadhir Vendhan: Concepts, Design, Definition of intellectual content, Literature search, Manuscript preparation, Manuscript Editing, and Manuscript review.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Cutaneous manifestations of metastatic Crohn's disease. Pediatr Dermatol. 2018;35:566-74.
- [CrossRef] [PubMed] [Google Scholar]
- Cutaneous manifestations of Crohn Disease. Dermatol Clin. 2015;33:417-31.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of Crohn's disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma: A pilot study. Tech Coloproctol. 2015;19:455-9.
- [CrossRef] [PubMed] [Google Scholar]
- The benefits of platelet-rich fibrin. Facial Plast Surg Clin North Am. 2019;27:331-40.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e45-50.
- [CrossRef] [PubMed] [Google Scholar]




