
Translate this page into:
Platelet Rich Plasma Combination Therapies for Treatment of Androgenetic Alopecia: A Systematic Review
Address for correspondence: Mr. Michael A. Kaiser, Dr. Phillip Frost Department of Dermatology and Cutaneous Surgery, University of Miami Miller, School of Medicine, 1600 NW 10th Ave #1140, Miami, FL 33136, USA. E-mail: mak320@med.miami.edu
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Androgenetic alopecia (AGA) is the most common cause of alopecia in males and females. Minoxidil and finasteride are the only FDA-approved treatments for AGA. New treatments including Platelet Rich Plasma (PRP) and microneedling have shown promising results. The purpose of this literature review was to highlight recent studies examining the effects of topical minoxidil combined with PRP to minoxidil or PRP monotherapy. The method used for this paper includes a systematic review of the literature from 2010 to 2022 using the PubMed, EMBASE, and MEDLINE databases examining studies evaluating combination therapies for AGA. Three randomized control trials compared combination PRP + topical 5% minoxidil to either no treatment, 5% minoxidil, or PRP only. Two studies found increased hair growth at five months and at six months following combined therapy. Another study found an increase in hair density and improved patient satisfaction with combination therapy compared to monotherapy. A prospective study revealed that patients treated with combined 5% minoxidil, PRP, and microneedling reported the highest patient and physician satisfaction compared to minoxidil monotherapy. An observational study evaluating topical 5% minoxidil with PRP reported an increase in hair diameter after one year of combination treatment compared to minoxidil monotherapy. PRP therapy combined with minoxidil and microneedling in a retrospective study was shown to increase hair growth compared to PRP with minoxidil as well as PRP or minoxidil monotherapy. In conclusion, a variety of studies demonstrated superior treatment response with a combination of PRP and minoxidil therapy in patients with AGA. Limitations to this study include different PRP preparation protocols, few randomized control studies, and small sample sizes.
Keywords
Androgenetic alopecia
microneedling
minoxidil
platelet rich plasma

INTRODUCTION
Male pattern hair loss (MPHL) and female pattern hair loss, also known as androgenetic alopecia (AGA), are the most common causes of alopecia in men and women, respectively.[1] The pathophysiology of AGA is thought to be rooted in hereditary and androgen dependent mechanisms. AGA is characterized by progressive thinning of terminal hairs to smaller, less visible vellus hairs.[23] In AGA, there is a gradual shortening of anagen phase reducing hair growth and length, and an increased telogen period leading to involution.[4] It is widely believed that androgens binding to the androgen receptor are the primary culprits in the alteration of hair cycle dynamics leading to progressive thinning and shortening of hair, and an increased number of hairs in the telogen phase.[5] These changes in the hair cycle dynamics lead to progressive thinning and shortening of hairs in the affected region ultimately culminating in the appearance of a bald spot. AGA in women typically affects the crown and bitemporal area while preserving the frontal hairline. Men with AGA also experience bitemporal hair loss with more involvement of the frontal hairline.[4]
Currently only minoxidil and finasteride are food and drug administration approved treatments for AGA. The mechanism of finasteride is through its inhibition of the type II 5a-reductase. Oral intake of 1 mg finasteride daily has been shown to reduce systemic levels of dihydrotestosterone and increase hair counts in AGA.[6] Minoxidil is traditionally a topical treatment for AGA, and opens adenosine triphosphate gated potassium channels in cell membranes leading to vasodilation, facilitating the progression to the G1 stage of the cell cycle of dermal papilla cells (DPCs), and ultimately improving hair growth through increased DPC proliferation and reduced dihydroxytestosterone (DHT) due to vasodilation.[78] Both treatments require long-term compliance and are associated with adverse effects that render long-term compliance difficult for many patients. Given the limitations of current food and drug administration approved treatments, other experimental treatments have been evaluated yielding promising results.
Experimental therapies for treating AGA include microneedling and platelet rich plasma (PRP). Microneedling involves using very fine needles to create micro abrasions in the skin. This process is thought to simulate WNT proteins and stem cells residing in the dermal papillae.[9] Studies have shown that microneedling alone can improve hair loss in AGA that is refractory to conventional treatment.[9] Microneedling has been shown to be effective as a monotherapy in patients who have failed conventional treatment.[10] The depth of penetration used in microneedling appears to play an important role in the overall therapeutic response. Faghihi et al.[11] compared combination therapy with minoxidil and microneedling at a depth of 1.2 mm to topical minoxidil with 0.6 mm depth of microneedling. The authors found that a superior clinical response was observed when using a depth of 0.6 mm for microneedling. In order for microneedling to be effective, an adequate depth must be achieved to puncture the papillary dermis in order to stimulate collagen production.[12] Most studies have demonstrated adequate treatment response with a depth of 1.5 mm.[913] Additionally there is speculation that despite the increased needle length, actual penetration might be substantially less than the maximum needle length which could account for the differences in efficacy seen in the literature.[14] Currently there is no established treatment protocol for optimal needle length and frequency of treatment. Given the low cost and low risk of adverse effects from microneedling, it remains a valuable tool in treating AGA. PRP is the volume of plasma fraction enriched with platelets from autologous blood obtained through centrifugation of a patient’s own venous blood. PRP has been examined in a variety of disease processes including tissue regeneration, wound healing and repair, and hair restoration.[15] PRP has been examined extensively in dermatology for applications in wound healing, facial augmentation, and scar remodeling.[16]
Role of platelet rich plasma in androgenetic alopecia
PRP has been shown to contain growth factors, chemokines, and cytokines which have been used for a variety of diseases including alopecia.[17] Among the most important factors in PRP are alpha granules produced and stored in platelets and contain platelet derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor beta, and insulin-like growth factors (IGF) all which are implicated in angiogenesis and the induction of stem cell differentiation and migration.[1618] PRP also comprises of dense granules which contain serotonin, histamine, calcium, and adenosine which contribute to improving membrane permeability and regulate inflammatory processes.[18] PRP is hypothesized to improve hair growth and limit hair follicle destruction by releasing large amounts of PDGF and other growth factors in the microenvironment reducing follicle apoptosis and promoting cell growth.[19] DHT has been implicated in MPHL and is thought to block the production of IGF-1. PRP contains IGF-1 and acts as an exogenous source of IGF-1 which can reduce the inhibitory effects of DHT on hair growth.[20]
The 2018 evidence-based (S3) guidelines for the treatment of AGA lists PRP therapy lowest as a potential treatment for AGA in both men and women.[21] The authors’ reasoning behind discouraging PRP as a meaningful intervention was based on limited studies available (only two studies using PRP met the inclusion criteria for men, whereas three studies were included for women), lack of control groups in the studies, and limited short-term follow-up. Notably, the 2018 S3 guidelines were the first to include PRP as a potential treatment, as in the 2011 guidelines PRP had not been evaluated as a potential treatment for AGA.[22] After the S3 guidelines were released, Gupta et al.[15] published a meta-analysis examining PRP as a potential therapy in AGA. PRP was shown to increase hair density compared to placebo and controls. Importantly, the lack of standardized PRP preparation protocols was discussed, as only two studies used the same protocol. A study by Ince et al.[23] attempted to compare autologous activated and non-activated PRP to homologous activated PRP for the treatment of AGA. The authors found that homologous PRP showed the greatest increase in hair diameter followed by non-activated autologous PRP. The authors suggested the potential for preparing PRP from pooled platelets with the same blood type as the patient could lead to superior results compared to autologous PRP preparation. A meta-analysis performed by Giordano et al.[17] examined randomized control trials evaluating the efficacy of PRP for the treatment of AGA demonstrated an increased hair number and cross sectional hair thickness compared to control groups. More recently, Verma et al.[24] directly compared PRP to topical minoxidil and found that PRP therapy yielded higher patient satisfaction and better clinical improvement compared to minoxidil. Whereas the individual effects of topical minoxidil and PRP have been examined in other studies, the focus of this review is to examine the current literature comparing combined topical minoxidil and PRP to monotherapy alone, as well as microneedling used in conjunction with PRP and topical minoxidil.
Recommendations for platelet rich plasma preparation
The National Indian Association of Dermatologists, Venereologists, and Leprologists (IADVL) PRP taskforce recommendations for PRP preparation attempted to address the lack of standardization of PRP protocols and highlight the salient, evidence-based methods of PRP preparation that were best suited for application in dermatology. The main recommendations from the IADVL include the use of a wide bore needle for drawing blood to prepare for PRP, the use of a double spin method, and recommended against activating PRP for its use in treating AGA.[25]
Literature search
A systematic review of the literature from 2010 to 2022 was performed in May 2022 using the PubMed, EMBASE, and MEDLINE databases [Figure 1]. Double blinded randomized controlled studies that assess the use of PRP and topical minoxidil in combination to treat AGA were included. Observational and retrospective studies that also examined microneedling with PRP and topical minoxidil were also included. The databases were searched using different combinations of the following keywords: platelet rich plasma, AGA, minoxidil, hair loss, microneedling, and PRP.
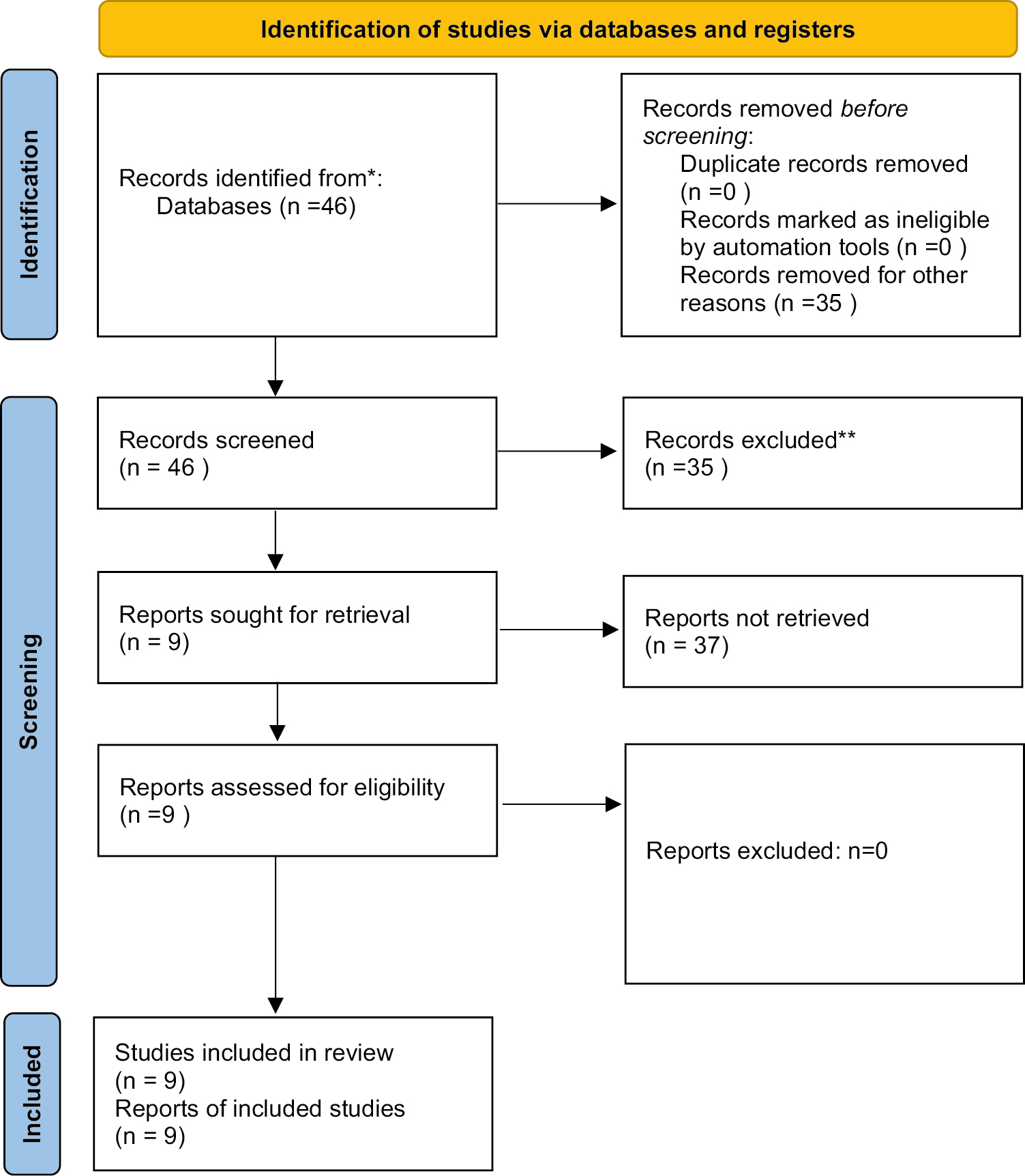
- Identification of appropriate studies for analysis. Flowchart depicting the exclusion processes for the identification of studies that are included this review
RESULTS
Randomized control trials
In total, five randomized control trials were published during the authors’ literature review. These studies compared combination PRP + topical 5% minoxidil to either a control group with no treatment, 5% minoxidil only treatment group, or PRP only group [Table 1].
| Reference | Patient population | Experimental groups | Assessment | Results |
|---|---|---|---|---|
| Alves and Grimalt[26] | 25 patients with AGA | Minoxidil split scalp: 13 patients treated with 1 mL 5% minoxidil twice daily and PRP (0.15–0.20 mL per injection, 4 mL total) in one half scalp; the other half injected with saline 3 months Finasteride split scalp: 12 patients with 1 mg/d oral finasteride and injections of pure PRP (0.15–0.20 mL per injection, 4 mL total) in one half scalp; other half was injected with saline for 3 months |
3 and 6 months Trichoscopy |
PRP led to significant increase in the hair count and hair density (P < 0.05) 6 months: Mean hair count, hair density, and terminal hair density showed significant positive effect in PRP and Minoxidil/Finasteride (P < 0.05) At 6 months: PRP/minoxidil showed superiority in mean hair count, hair density compared to PRP/finasteride (P < 0.05) |
| Pakhomova and Smirnova[27] | 69 men with AGA | PRP only: 22 patients received PRP (4 mL injected into the scalp, 0.15 mL per injection), every month for 4 months Combined: 25 patients received 5% minoxidil with PRP injection (4 mL was injected into the scalp 0.15 mL per injection), every month for 4 months Minoxidil only: 22 patients received 5% minoxidil alone |
4 months Trichoscopy |
Combined therapy: Significant improvement in hair density in eight patients (36%) Minoxidil: Significant improvement in hair density in four patients (18%) PRP: An improvement in hair density in nine people (36%). Combined therapy exceeded the effects of PRP only in hair density by 2.9 times (P = 0.0001) |
| Kumar Singh et al.[28] | 80 patients with AGA | Minoxidil only: 5% Minoxidil topically 1 mL twice/day Minoxidil and PRP: 5% Minoxidil topically 1 mL twice/day and PRP monthly for 3 months NS control PRP only: PRP monthly for 3 months |
1, 2, 3, 4, 5 months Clinical photography, Hair density |
Minoxidil with PRP had highest patient satisfaction followed by PRP alone Increase in hair density was largest in Minoxidil with PRP |
| Ramadan et al.[30] | 126 patients with AA | 5% Minoxidil + hormonal therapy (Spironolactone for women, Finasteride for Men) + PRP (0.1 mL PRP, 1 cm deep) 5% Minoxidil + hormonal therapy (Spironolactone for women, Finasteride for Men), Microneedling (dermapen, depth of 2 mm and frequency of 3) + PRP (0.1 mL PRP, 1 cm deep) |
3 and 6 months Digital dermoscopy |
PRP + microneedling: greatest improvement (78.3 ± 10.6) PRP alone: improvement of (64.3 ± 14.3) |
| Tan et al.[29] | 16 men patients with AGA (split scalp) | Minoxidil + concentrated growth factors (CGF): 16 patients half scalp (0.1 mL/cm2) every 4 weeks (three sessions) Minoxidil only: 16 patients half scalp |
4, 8, 12, 24 weeks Hair density and trichoscopy |
Minoxidil + CGF: Hair growth ratio at 12 weeks was higher than Minoxidil only (P < 0.01), hair density and efficacy was also greater |
Alves and Grimalt[26] examined 13 men and women patients with AGA in a randomized double blinded placebo controlled half-head study. Half the scalp was treated with 1 mL of 5% topical minoxidil solution twice daily with PRP injection and the other half of the scalp with 1 mL of 5% topical minoxidil solution twice daily and injected saline for placebo. PRP injection was performed in 4 pre-selected areas (2 areas in each half-head of the scalp: one frontal and one occipital). 4 mL total of PRP was administered as 0.15–0.20 mL per point of injection. PRP injections were administered once a month for 3 months. Evaluation criteria consisted of Trichoscan analysis using the Fotofinder system and professional version. Patients were evaluated at baseline, 1 month after treatment, 2 months after treatment, and at 6-month follow-up. The authors found that PRP with minoxidil 5% solution applied twice daily increased mean hair count (P < 0.0105) and increased mean hair density (P < 0.0104) compared to minoxidil monotherapy applied twice daily. The effect of the combination therapy was most profound at the 6-month interval. This study had adequate controls and parameters to reduce bias. A longer follow-up period to assess the combined effects of both minoxidil and PRP would have added value to this study. Minoxidil is known to cause a reversible period of hair shedding early on in treatment and this could have negatively impacted the results early in the clinical trial. The overall study design was strong given the investigators were double blinded and the 6-month follow-up period was longer than many other studies.
Pakhomova and Smirnova[27] performed a randomized double blinded placebo-controlled trial evaluating monotherapy versus combined therapy of PRP with topical 5% minoxidil in 69 men patients with AGA. The authors evaluated clinical efficacy through the dynamics of morphometric hairs and trichoscopy. Cell proliferation in skin biopsies was evaluated through antibodies to beta-catenin, CD34, Ki67, and to Dkk-1. In the combined PRP with 5% minoxidil group, hair density increased by 32% (P < 0.00004), mean hair diameter increased, and there was a decrease in proportion of vellus hairs by 30% (P < 0.00082). Overall, combination treatment increased hair density by 2.9 times compared to PRP monotherapy (P = 0.0001) and increased hair density 1.74 times compared to minoxidil monotherapy (P = 0.0347). PRP treatment was shown to increase both beta-catenin and the CD34 expression area and there was an increase in the Ki67+ index. One of the main advantages of this study is the comparison of PRP alone to PRP combination therapy and minoxidil monotherapy. The authors note in their study that the short follow-up time was a deficiency in their study especially since the effects of minoxidil can be delayed up to 8 or even 12 months. The authors also noted in their study the effects of PRP also had a delayed onset further compounding the issue with the relatively short 4-month follow-up period. Studies with longer follow-up time require more resources and funding and this study may provide the evidence needed to complete a longer study.
Singh et al. performed a randomized double blinded placebo-controlled trial evaluating 80 men patients with AGA stratified into four treatment groups.[28] Group I contained 20 patients who applied topical 5% minoxidil 1 mL twice daily and monthly normal saline injections for 3 months. Group II contained 20 patients who applied topical 5% minoxidil 1 mL twice daily and monthly PRP injections for 3 months. Group III contained 20 patients applied a topical placebo twice a day and received normal saline injections monthly for 3 months, and Group IV contained 20 patients who applied topical placebo twice a daily and received monthly PRP injections for 3 months. Patients were evaluated at six intervals: baseline and monthly for a total of 5 months. Intervention efficacy was assessed through hair density through dermoscopy, clinical photography, and patient self-assessment. Patient self-assessment score was recorded based on a rating scale of 0–4. A score of 0 represented no improvement whereas a score of 4 represented 76%–100% improvement. Maximum efficacy was observed in Group II (combination treatment group) which saw the highest increase in mean hair density (P < 0.0001) compared to monotherapy (PRP or minoxidil) + placebo and double-placebo groups. Group II also reported the highest patient self-satisfaction score. This study has a strong experimental design using double blinded and double placebo controls. Similarly, to the previous studies examined, the sample size was small and the follow-up time was relatively short at 2 months following the final PRP procedure.
Tan et al.[29] performed a similar split scalp randomized double blinded placebo controlled clinical trial examining topical 5% minoxidil with concentrated growth factor (CGF). CGF differs from PRP in that during the isolation process CGF is collected through single-spin centrifugation at continuous variable speed of patient’s autologous whole blood. The mechanism of preparation of PRP is often done using two spin centrifugations of autologous whole blood, but collection protocols vary widely. The authors report that CGF contains higher concentrations of factors promoting angiogenesis such as FGF and VEGF compared to PRP. A total of 16 men patients with AGA were divided into two groups, a minoxidil with CGF group and a minoxidil only group. Minoxidil was applied twice a day on both sides of the scalp for the 24 weeks. CGF was applied once a month for 3 months to half the scalp and saline placebo was applied to half the scalp in the minoxidil monotherapy group. The patients were evaluated at baseline, 4 weeks, 8 weeks, 12 weeks, and 24 weeks. Treatment efficacy was evaluated using trichophotography using a dermatoscope for measuring hair count, hair density, and the hair growth ratio (calculated as the hair growth at 12 weeks compared to baseline). Overall, the authors found the combined minoxidil with CGF group to have a higher hair growth ratio compared to minoxidil monotherapy (P < 0.01). Additionally, hair density in the combined group was greater than the minoxidil monotherapy (P < 0.05). Notably the authors did not include a CGF monotherapy group in their study. The clinicians were double blinded in the study reducing risk of bias and strengthening the integrity of the study. Unfortunately, the sample size was only 16 patients, but this study serves as a strong starting point to evaluate combination therapy.
Ramadan et al.[30] performed a single blinded randomized control study evaluating 126 patients (46 men and 80 women) with AGA. All patients received combined treatment of PRP with topical 5% minoxidil daily, once a day for women patients and twice a day for men patients. Additionally, women patients received 100 mg daily of spironolactone whereas men received 2.5 mg of daily finasteride. 42 patients received direct PRP combined with topical minoxidil and oral hormonal therapy. 42 patients received automated microneedling and PRP combined with topical minoxidil and oral therapy. PRP scalp injections occurred in areas of alopecia and consisted of 0.1 mL of PRP injected 1 cm deep in the scalp. Evaluation of treatment efficacy was measured through digital dermoscopy measuring changes in hair density and hair diameter at 6 months after the first PRP session. The combined microneedling with PRP, topical minoxidil, and oral hormonal therapy group demonstrated the greatest increase in hair density and mean hair diameter (P < 0.001) compared to the control group and the PRP plus minoxidil and oral hormonal treatment group. This study had a good experimental design, although with men and women undergoing different therapies, it is difficult to attribute one treatment as the reason for overall improvement especially in a study with limited sample size. Nevertheless, the results do show that microneedling and PRP may confer a therapeutic advantage over traditional therapy.
Observational studies
Ray et al.[31] performed an observational study examining 100 patients with AGA [Table 2]. 50 patients received topical 5% minoxidil lotion daily for 12 months combined with six PRP injections at monthly intervals and 50 patients received topical 5% minoxidil for 12 months alone. 1 mL of minoxidil was applied twice daily. Assessment of clinical response was completed using trichoscopy evaluating hair density and mean hair diameter. Results were evaluated at 1 year follow-up after continuous therapy. The authors noted that 100% of patients in the combination group noted some degree of improvement whereas 87% of patients with minoxidil monotherapy did. Additionally, mean hair diameter in the combination group was significantly greater compared to minoxidil monotherapy (P < 0.05). This study provides valuable data for treatment response after long-term follow. Many of the studies discussed in this review were not able to follow patients for long periods of time. Although the clinicians were not blinded, this study presents important data that PRP in combination with minoxidil can yield superior results. A third arm of the study comparing PRP monotherapy would have been a valuable addition to the study.
| Reference | Patient population | Experimental groups | Assessment | Results |
|---|---|---|---|---|
| Ray and Sharma[31] | 200 men with AGA (10 patients lost) | Group A: 100 patients with topical 5% minoxidil for 12 months Group B: received combination therapy of PRP (6 injections at monthly intervals) and topical 5% Minoxidil for 12 months |
1 year Trichoscopy |
Group A: 87% of patients showed moderate to great improvement, greater improvement in hair density Group B: 60% of patients showed moderate to great improvement |
| Shah et al.[13] | 50 patients with AGA | Group A: 5% topical minoxidil (1 mL twice daily) Group B: 5% topical minoxidil (1 mL twice daily) + microneedling (1.5 mm depth 8 times in each direction) + PRP (6 sessions at monthly intervals) |
6-month Serial photographs and patient and clinician assessment |
Group B showed improvement in patients’ assessment at 6 months compared to Group A (P < 0.05) Group B showed improvement in clinicians’ assessment at 6 months compared to Group A (P < 0.05) |
| Jha et al.[35] | 93 patients with AGA | Minoxidil only: minoxidil 5% lotion twice daily (n = 31) Minoxidil and PRP (1 mL, 3-week intervals, 4 sessions) (n = 31) Minoxidil with PRP (1 mL, 3-week intervals, four sessions) and microneedling (number of needles—192, size—1.5 mm, until pinpoint bleeding) (n = 31) Placebo: normal saline |
3 months Serial photographs |
Group 3 had highest patient satisfaction followed by Group 2 and Group 1 |
Ho et al.[32] performed a retrospective study examining 24 patients with AGA taking combined PRP and minoxidil. 20 out of 24 patients also took oral antiandrogen therapy. Patients were followed for 2 months after initial PRP injection and continued to follow-up for a maximum of 6 months. Patients also received additional PRP injections between 3 and 4 months of follow-up. A statistically significant increase in hair diameter was seen in 71% of patients at 2 months of follow-up. Nearly 63% of patients experienced greater than ten percent hair regrowth, whereas nearly 34% of patients experienced an increase in hair regrowth greater than 20%. Whereas the results appear encouraging, this study had several major shortcomings including no control groups, patients with differing oral androgen medications, and no blinding. The 6-month follow-up period was longer than many other published studies and demonstrated encouraging results but given the major flaws in experimental design it is difficult to draw meaningful conclusions and apply that to the general population.
Pachar et al.[33] performed a comparative split scalp study of 50 men patients with AGA. One side of the scalp was treated with minoxidil only and the other side of the scalp was treated with PRP and 1 mL of topical minoxidil twice per day. Patients were evaluated at 6 months after PRP injection and sustained minoxidil use. Patients reported increased self-satisfaction scores on the PRP and minoxidil side compared to the minoxidil monotherapy side. Importantly, fewer patients reported side effects in the PRP+ minoxidil group compared to the minoxidil side of the scalp. A statistically significant increase in hair density was seen in the combined group compared to minoxidil monotherapy. The authors did not report on whether the greater increase in hair density in the combined group compared to the minoxidil monotherapy was statistically significant. Additionally, there was no placebo group and no blinding of the clinicians. This study serves has more evidence that combined therapy with PRP and minoxidil may be beneficial, but future studies should have a stronger experimental design.
PRP therapy with microneedling and minoxidil
Shah et al.[13] performed an open prospective study evaluating 50 patients with AGA. 25 patients were treated with topical 5% minoxidil alone (1 mL twice daily), and 25 patients were treated with topical minoxidil, microneedling, and PRP injection. Microneedling was done using a dermaroller with needle length of 1.5 mm eight times in each direction until mild erythema was appreciated. Microneedling was followed by PRP injections with 0.05 mL per 1 cm2. Microneedling with PRP injection occurred monthly for 6 months with continued topical minoxidil treatment. Patients were evaluated at baseline and at 6 months with both self-satisfaction and physician satisfaction. Investigators reported the highest improvement in the combination group (P < 0.05) compared to monotherapy. Additionally, patient satisfaction was higher in the combination group compared to monotherapy (P < 0.05). Whereas there was no control group or blinding of the clinicians, this observational study does add to the existing body of knowledge regarding combination therapy and serves as one of the first studies examining microneedling with PRP and minoxidil.
Yepuri and Venkataram[34] enrolled 60 patients with AGA who failed to respond to minoxidil or finasteride and evaluated their response to PRP with microneedling. All patients received PRP treatment and microneedling between four and six times at an interval of 4 weeks. 5 mL of PRP were aliquoted into 1 mL insulin syringes and applied to the treatment area. Microneedling was done using a dermaroller with 1.5 mm needles in all directions. Patients were assessed at baseline, after each treatment session, 4 weeks after the final treatment session, and at 3 and 6 months after the final treatment session. Clinical improvement was measured through clinical photographs of the scalp taken at each session and at follow-up as well as subjective patient satisfaction scores. 82% of patients in the study had at least 40% improvement compared to baseline in hair thickness and growth. Only 6% of patients reported poor response to the treatment. Whereas on the surface the results appear promising, lack of blinding and lack of controls are deficits of the experimental design. One positive note is that all patients had previously failed conventional treatment with minoxidil or finasteride and nearly all patients subsequently benefited from PRP with microneedling in this study. More objective criteria for evaluating hair growth such as measuring hair density and thickness through trichoscopy would have been valuable tools in adequately characterizing hair regrowth. Another important takeaway is that the authors found that adequate treatment response was able to be achieved after four total sessions which can aid in the development of future treatment protocols for AGA.
As microneedling is now more frequently utilized in conjunction with PRP therapy (topical application and/or injections), we further sought studies that included this modality as it more accurately reflects real-world treatment paradigms. Jha et al.[35] performed a retrospective study evaluating 93 patients with AGA stratified into three treatment groups. Group A consisted of 31 patients treated with 5% topical minoxidil monotherapy twice daily, Group B contained 31 patients who were treated with PRP and 5% topical minoxidil twice daily, and Group C contained 31 patients who received PRP, 5% topical minoxidil twice daily, and microneedling. Microneedling occurred using 192 needles, size 1.5 mm, and was performed until pinpoint bleeding occurred. PRP treatment contained 1 mL of PRP and was injected into the scalp at 3-week intervals for a total of four sessions. Patients were evaluated at baseline and at 3-month follow-up after treatment. Clinical efficacy was evaluated using hair pull test and dermoscopy evaluating number of terminal hair follicles. Group C had the highest number of negative hair pull tests followed by group B (P < 0.05), and Group C had the highest terminal to vellus ratio, followed by group B (P < 0.046). The authors concluded that it appeared that microneedling in combination with PRP and topical minoxidil had the most improvement in hair growth outperforming PRP with topical minoxidil as well as minoxidil monotherapy.
DISCUSSION
The purpose of this review is to highlight the growing evidence for using PRP and minoxidil combination therapy to treat AGA. The majority of these studies were published between 2018 and 2022 suggesting the relative infancy of the clinical evaluation of combination therapy. In this review PRP combined with topical minoxidil generally and consistently demonstrated positive results in treating AGA, both from objective hair-centric quantification methods as well as patient- and physician-reported measurements. This combination therapy represents an exciting opportunity to enhance the therapeutic response to minoxidil, which is the anchor of AGA and many other alopecic conditions. Whereas early studies demonstrate potentially promising results, there is still considerable evaluation that is required. Currently there are many protocols for producing PRP and this represents a major obstacle to adequately evaluate the results of these studies. Given that different centrifuge column manufacturers exist with their own protocols, it will be imperative to perform cross-protocol studies. Limitations to the randomized control studies referenced in this review were short follow-up time, varied PRP preparation protocols, and small sample sizes. More rigorous clinical trials with larger patient groups and longer follow-up are required to adequately analyze the therapeutic response of PRP and minoxidil combination therapy. Additionally, many of these studies were observational studies without double blinded experimenters and lacked objective data to measure therapeutic response.
Topical minoxidil is a vasodilatory drug that increases prostaglandin E2 in the hair follicle increasing the length of anagen phase and hair follicle size.[36] Minoxidil is known to cause adverse effects including scalp erythema, pruritis, dryness, scaling, and hypertrichosis.[3738] Among these adverse effects, hypertrichosis, which is due to the medication typically dripping down the forehead, temples and cheeks, poses the most challenging obstacle in achieving long-term compliance. A meta-analysis by Gupta et al.[39] found that when clinical evidence of improvement was present in most patients with AGA being treated with topical minoxidil, few patients reported cosmetically acceptable results. The authors also discussed compliance as the major barrier to long-term treatment. However, with the resurgence of low dose oral minoxidil, compliance is less of a concern and may provide even further benefit in combination therapy with PRP.[40]
PRP has been examined in a variety of medical conditions including AGA. It contains large amounts of growth factors and it has been hypothesized that growth factors produced by platelets can induce stem cell in the hair follicle to differentiate and produce new follicles.[41] PRP is prepared from autologous centrifugation of the patient’s blood eliminating risk of adverse reaction to the product itself. Currently there are many different isolation methods for PRP, although there are four families of preparation protocols based on patient leukocyte count and fibrin architecture.[42] Cervantes et al.[42] published a meta-analysis examining the effects of PRP in AGA and found that ten out of 12 studies evaluated reported positive results with PRP. Very few adverse effects were noted although some patients noted mild headache, desquamation, and transient edema. Given the favorable side effect profile of PRP and the ability to spread out treatments over periods of weeks or months long-term compliance is greater.
Microneedling was the final treatment modality used in several of the referenced studies in combination with PRP and minoxidil. Microneedling is a minimally invasive procedure using very small gauge needles to create micropunctures in the epidermis leading to neovascularization, growth factor release, and expression of factors promoting growth cycle progression.[943] Microneedling is believed to promote hair restoration in alopecia through promoting local release of PDGF, VEGF, and endothelial growth factor acting on the hair bulge.[43] The studies that used microneedling in conjunction with PRP demonstrated enhanced regrowth of hair, likely due to both modalities promoting local growth factor release. Major advantages to microneedling include the low cost of treatment and minimal adverse effects.
In real-world treatment scenarios for AGA, patients are more likely to undergo multi-modal combination therapy beyond minoxidil, PRP and microneedling. Other treatments added into the mix include anti-androgens such finasteride and spironolactone as well as vitamins/supplements including saw palmetto and pumpkin seed extract.[44] Naturally, it will be of benefit to compare these multi-combinatorial treatments to the PRP+minoxidil combination therapy highlighted here.
CONCLUSION
Given the current body of existing evidence examining PRP for the treatment of AGA, there is strong evidence to support PRP as a potential therapeutic option. Combined PRP with minoxidil or microneedling increased hair density and hair diameter compared to monotherapy. The major limitations to establishing PRP as a treatment option in AGA are short follow-up times in the current body of evidence and lack of strong experimental design. Combination therapy with PRP with minoxidil yielded better results in most studies. Minoxidil can take up to 8 months for the therapeutic effect to be realized which is a barrier to long-term adherence of minoxidil therapy. Studies show that PRP may confer an early therapeutic benefit before the effects of minoxidil can be fully realized. Patients should be counseled on the therapeutic benefit of PRP as an adjunctive treatment in AGA. Whereas PRP is a more invasive and costly procedure with a small risk of infection, the early treatment benefit and potential for synergy with minoxidil may be appealing to patients. The luxury of PRP is that it can be used orthogonally in the treatment of AGA. PRP is generally a more expensive procedure than topical minoxidil, and patients should be counseled on the potential economic burden prior to pursuing PRP. Not all patients are candidates for PRP, and it should be avoided in patients with a history of malignancy, platelet disorders, anemia, bleeding disorders, or patients who are immunocompromised.[19] Additionally, PRP with microneedling represents a viable treatment option in patients who have failed minoxidil treatment. In the past 4 years, much stronger evidence for the use of PRP in combination with other conventional therapies has emerged, but before it can become standard of care longer follow-up times and larger patient populations in studies are required to understand the long-term advantage of PRP therapy. Whereas there are encouraging results, a standardized protocol use for PRP isolation must be adopted to adequately evaluate PRP as a treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Androgenetic alopecia: An update. Indian J Dermatol Venereol Leprol. 2013;79:613-25.
- [Google Scholar]
- Androgenetic alopecia: Pathogenesis and potential for therapy. Expert Rev Mol Med. 2002;4:1-11.
- [Google Scholar]
- Examining the safety and efficacy of low-level laser therapy for male and female pattern hair loss: A review of the literature. Skin Appendage Disord. 2020;6:259-67.
- [Google Scholar]
- Medical treatments for male and female pattern hair loss. J Am Acad Dermatol. 2008;59:547-66. quiz 567
- [Google Scholar]
- A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: A pilot study. Int J Trichol. 2013;5:6-11.
- [Google Scholar]
- Response to microneedling treatment in men with androgenetic alopecia who failed to respond to conventional therapy. Indian J Dermatol. 2015;60:260-3.
- [Google Scholar]
- Microneedling in androgenetic alopecia; comparing two different depths of microneedles. J Cosmet Dermatol. 2021;20:1241-7.
- [Google Scholar]
- Micro needling: A novel therapeutic approach for androgenetic alopecia. A review of literature. Dermatol Ther. 2020;33:e14267.
- [Google Scholar]
- A comparative study of microneedling with platelet-rich plasma plus topical minoxidil (5%) and topical minoxidil (5%) alone in androgenetic alopecia. Int J Trichol. 2017;9:14-8.
- [Google Scholar]
- A comprehensive review of microneedling as a potential treatment option for androgenetic alopecia. Aesthetic Plast Surg. 2022;1
- [Google Scholar]
- Platelet-rich plasma as a treatment for androgenetic alopecia. Dermatol Surg. 2019;45:1262-73.
- [Google Scholar]
- Platelet-rich plasma (PRP): Current applications in dermatology. Skin Therapy Lett. 2019;24:1-6.
- [Google Scholar]
- Platelet-rich plasma for androgenetic alopecia: Does it work? Evidence from meta analysis. J Cosmet Dermatol. 2017;16:374-81.
- [Google Scholar]
- Systematic review of the use of platelet-rich plasma in aesthetic dermatology. J Cosmet Dermatol. 2015;14:315-23.
- [Google Scholar]
- Efficacy of platelet-rich plasma in treatment of androgenic alopecia. Asian J Transfus Sci. 2015;9:159-62.
- [Google Scholar]
- A mechanistic model of platelet-rich plasma treatment for androgenetic alopecia. Dermatol Surg. 2016;42:1335-9.
- [Google Scholar]
- Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men—Short version. J Eur Acad Dermatol Venereol. 2018;32:11-22.
- [Google Scholar]
- Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. JDDG. 2011;9:S1-S57.
- [Google Scholar]
- Comparison of the efficacy of homologous and autologous platelet-rich plasma (PRP) for treating androgenic alopecia. Aesthetic Plast Surg. 2018;42:297-303.
- [Google Scholar]
- A study to compare the efficacy of platelet-rich plasma and minoxidil therapy for the treatment of androgenetic alopecia. Int J Trichol. 2019;11:68-79.
- [Google Scholar]
- Preparation of platelet-rich plasma: National IADVL PRP taskforce recommendations. Indian Dermatol Online J. 2021;12:12S12.
- [Google Scholar]
- Platelet-rich plasma in combination with 5% minoxidil topical solution and 1 mg oral finasteride for the treatment of androgenetic alopecia: A randomized placebo-controlled, double-blind, half-head study. Dermatol Surg. 2018;44:126-30.
- [Google Scholar]
- Comparative evaluation of the clinical efficacy of prp-therapy, minoxidil, and their combination with immunohistochemical study of the dynamics of cell proliferation in the treatment of men with androgenetic alopecia. Int J Molec Sci. 2020;21:65166516.
- [Google Scholar]
- Comparison of efficacy of platelet-rich plasma therapy with or without topical 5% minoxidil in male-type baldness: A randomized, double-blind placebo control trial. Indian J Dermatol Venereol Leprol. 2020;86:150-7.
- [Google Scholar]
- Autologous concentrated growth factors combined with topical minoxidil for the treatment of male androgenetic alopecia: A randomized controlled clinical trial. Facial Plast Surg Aesth Med. 2021;23:255-62.
- [Google Scholar]
- Evaluation of adding platelet-rich plasma to combined medical therapy in androgenetic alopecia. J Cosmet Dermatol. 2021;20:1427-34.
- [Google Scholar]
- Comparison of 5% minoxidil lotion monotherapy versus its combination with autologous platelet rich plasma in androgenetic alopecia in hundred males. Med J Armed Forces India. 2021;77:355-62.
- [Google Scholar]
- Trichologic response of platelet-rich plasma in androgenetic alopecia is maintained during combination therapy. J Am Acad Dermatol. 2020;82:478-9.
- [Google Scholar]
- A comparative study of efficacy of 5% minoxidil and 5% minoxidil plus platelet-rich plasma in same patient for treatment of androgenetic alopecia. J Cutaneous Aesthetic Surg. 2022;15:71-6.
- [Google Scholar]
- Platelet-rich plasma with microneedling in androgenetic alopecia: Study of efficacy of the treatment and the number of sessions required. J Cutan Aesthet Surg. 2021;14:184-90.
- [Google Scholar]
- Platelet-rich plasma and microneedling improves hair growth in patients ofandrogenetic alopecia when used as an adjuvant to minoxidil. J Cosmet Dermatol. 2019;18:1330-5.
- [Google Scholar]
- Management of androgenetic alopecia: A comparative clinical study between plasma rich in growth factors and topical minoxidil. Eur J Plastic Surg. 2016;39:173-80.
- [Google Scholar]
- Allergic contact dermatitis to topical minoxidil solution: Etiology and treatment. J Am Acad Dermatol. 2002;46:309-12.
- [Google Scholar]
- Minoxidil and its use in hair disorders: A review. Drug Des Develop Ther. 2019;13:2777-86.
- [Google Scholar]
- Topical minoxidil: Systematic review and meta-analysis of its efficacy in androgenetic alopecia. Skinmed. 2015;13:185-9.
- [Google Scholar]
- Oral minoxidil treatment for hair loss: A review of efficacy and safety. J Am Acad Dermatol. 2021;84:737-46.
- [Google Scholar]
- Platelet-rich plasma in androgenic alopecia: Myth or an effective tool. J Cutaneous Aesthet Surg. 2014;7:107-10.
- [Google Scholar]
- Effectiveness of platelet-rich plasma for androgenetic alopecia: A review of the literature. Skin Appendage Disord. 2018;4:1-11.
- [Google Scholar]
- Microneedling for the treatment of hair loss? J Eur Acad Dermatol Venereol. 2018;32: 564-9.
- [Google Scholar]
- An overview of herbal alternatives in androgenetic alopecia. J Cosmet Dermatol. 2019;18:966-75.
- [Google Scholar]




