
Translate this page into:
Self-made insulated needle

*Corresponding author: Dr. Yogesh Bhingradia. Chief Consultant, Shivani Skin Care and Cosmetic Clinic, Surat, Gujarat, India. yogeshbhingradia@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhingradia YM, Patel N. Self-made insulated needle. J Cutan Aesthet Surg. doi: 10.25259/jcas_7_24
Abstract
Radiofrequency (RF) ablation is a surgical procedure which uses alternating current at ultra-high frequency for controlled tissue destruction. The wide range of dermatological indications includes the management of benign and malignant skin lesions. Certain skin conditions where the target tissue is deeper and epidermal sparing is required such as leukotrichia, trichiasis, cherry angioma, infantile hemangioma, and angioma serpiginosum need more precise energy delivery. These conditions can be addressed by insulated RF for localized tissue destruction without damaging the surface/epidermis and hence reducing the side effects such as post-inflammatory hyper or hypopigmentation and scarring. A simple, non-expensive, commercially available adhesive can be used to coat the normal RF needle for safe cauterization and good cosmetic outcomes.
Keywords
Insulated needles
Non-insulated needles
Radiofrequency

INTRODUCTION
Radiofrequency (RF) ablation is a surgical procedure which uses alternating current at ultra-high frequency for controlled tissue destruction. The wide range of dermatological indications includes the management of benign and malignant skin lesions such as verruca, molluscum contagiosum, pyogenic granuloma, actinic keratoses, and xanthelasma. Non-insulated needle emits RF energy over the entire surface of skin, i.e., epidermis and dermis, thus allowing all the layers to be heated at once which may further increase the probability of surface changes such as pigmentation and scar formation.1
Certain skin conditions where the target tissue is deeper and epidermal sparing is required such as leukotrichia, trichiasis, cherry angioma, infantile hemangioma, and angioma serpiginosum need more precise energy delivery. Anderson and Parrish changed the concept of treating cutaneous vascular lesions by introducing selective photo thermolysis in 1983.2,3
These conditions can be addressed by insulated RF for localized tissue destruction without damaging the surface/epidermis and hence reducing the side effects such as post-inflammatory hyper or hypopigmentation and scarring.
The insulated needle only delivers energy at the tip of the needle, preventing heat from dispersing into the surrounding area. This modification of the needle by insulation decreases the recovery time as the necrosis is lesser than non-insulated needle. There are multiple, commercially available insulated needles; but to alleviate the problem of its expense, the author has been researching and developing its alternative for years.
CASE REPORT
A total of 15 patients were included in our study from 2 years of age to 70 years of age. We decided to use a self-made insulated needle made by the author to conduct this study to find out the efficacy of the RF needle. The tip of the RF needle was thoroughly cleaned with spirit after which a thin layer of cyanoacrylate glue was applied throughout the length of needle in a circumferential manner leaving behind only 2–3 mm of the tip area which will act as a conducting system at the time of treatment. Hence, this simple pre-procedure step will make a non-insulated needle into an insulated one [Figure 1].
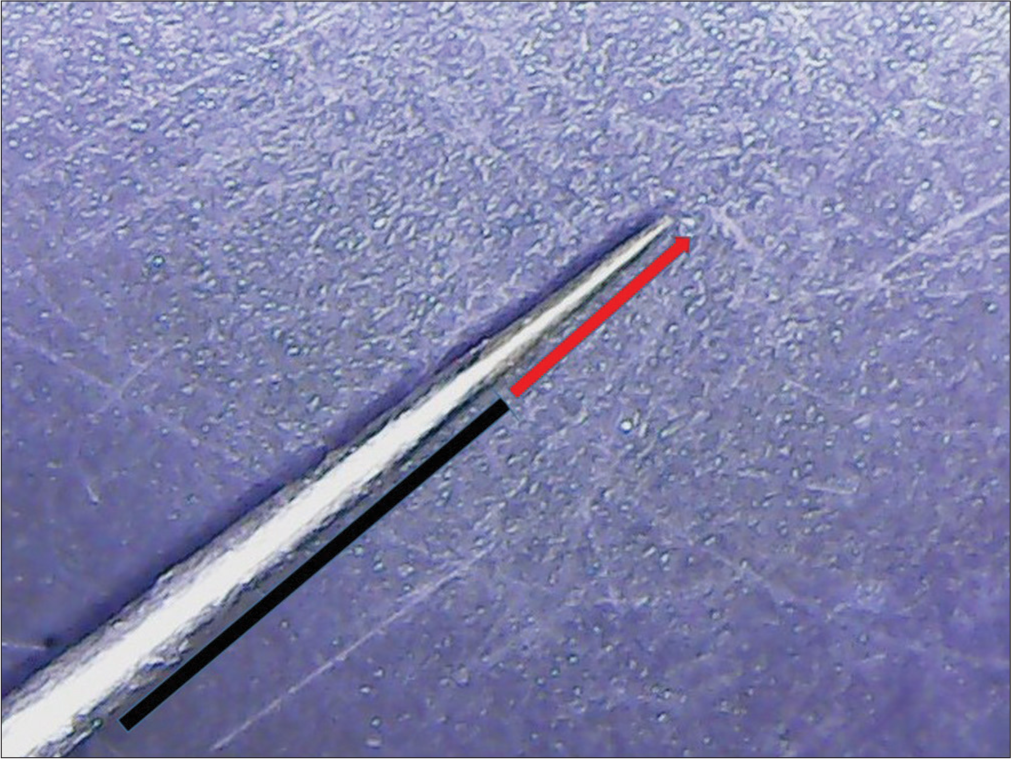
- Self-made insulated needle. The red arrow is a non insulated part of RF needle and the black line indicates the insulated part.
After written informed consent, digital photographs were taken. A topical anesthetic agent was applied on the affected area 45 min before the procedure. After stretching the skin with the help of fingers, the needle is inserted just beneath the base of the lesion and the RF energy is delivered at the lesion base.
This RF method was used for multiple indications in our study. Herein, we present a series of 30 cases that were treated using non-insulated needle and self-made insulated needle with excellent cosmetic outcomes. The indications include (1) leukotrichia [Figure 2a and b], (2) trichiasis [Figure 3a and b], (3) cherry angioma, (4) infantile hemangioma, and (5) venous lake.
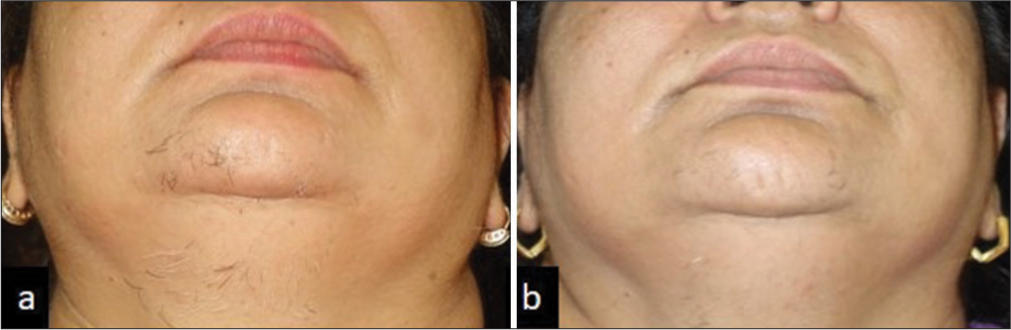
- (a and b) Pre and post procedure pictures of leukotrichia treated with self-made insulated needle.
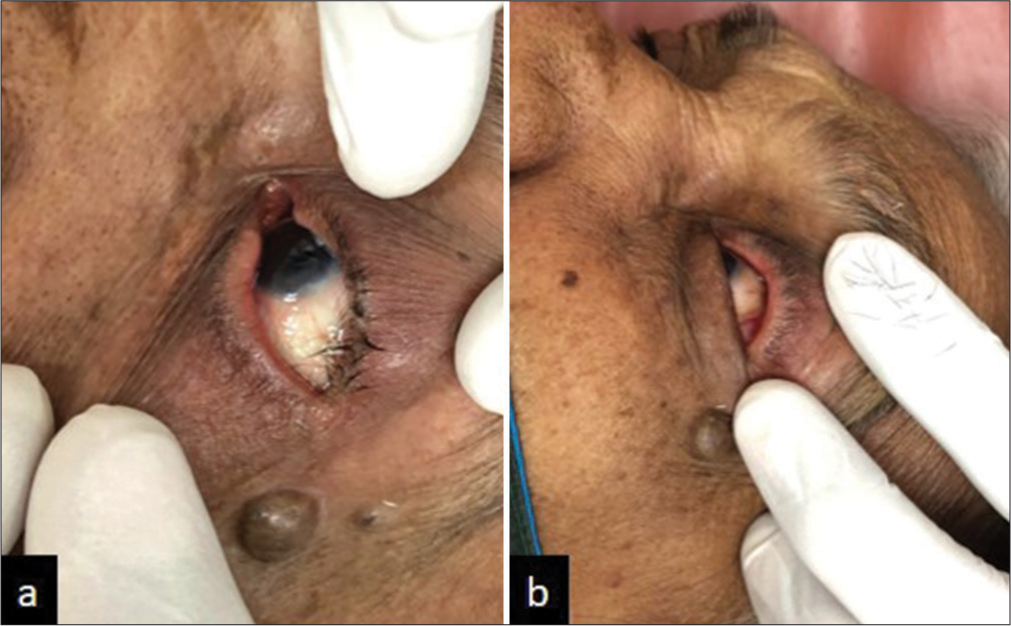
- (a and b) Pre and post-procedure pictures of trichiasis treated with self-made insulated needle.
DISCUSSION
The lesion site was assessed after 6 weeks of initial treatment for any side effects. Of 30 patients treated, 50% of patients were treated using insulated needle and rest were treated with non-insulated needle. The mean age of patients in group 1 was 32.5 years and that in group 2 was 35 years of age. A total of 5 indications were treated in both groups equally of which the most common one was hypertrichosis (33.3%), followed by venous lake and cherry angioma (20%), trichiasis (13.3%), and infantile hemangioma and spider nevi (6.6%) each. Both the groups were assessed after 6 weeks of RF and the side effects in group 1 were 0%, while all the patients in group 2 showed some degree of hyperpigmentation (100%). There are various treatments to treat all the above indications such as carbon dioxide laser, cryotherapy, and electroepilation, but cosmetic concerns from epidermal injury and lower efficacy rate due to the incomplete destruction of deep dermal lesions are not much improved.
The insulated needle is the solution to all the above-mentioned cosmetic concerns, but its marketed cost has always been its biggest disadvantage in the Indian market. Hence, to overcome this difficulty, the author here invented a self-made insulated needle using a 5-rupee fevikwik. The insulation was at the base of the needle, while its tip was non-insulated. That way, the needle selectively destroyed the dermal component of the lesion without harming the epidermis. After treatment with RF, both the groups of patients showed marked reduction in the lesions size and number. The cosmetic outcome of Group 1 patients was excellent on top of the needle efficacy.
CONCLUSION
The advantage of our insulated needle over the commercially available needles is that the commercially available needles provide specific length of insulation which cannot be varied. On the contrary, the author’s technique allows the dermatologist to assess the depth of the lesion and thus can decide the length of insulation needed in each specific lesion to gain the optimum result. This flexible insulating technique opens a wide range of indications for a dermatologist to treat, which would have been avoided otherwise. A simple, non-expensive, commercially available adhesive can be used to coat the normal RF needle for safe cauterization and good cosmetic outcomes.
Authors’ contributions
The concept was by the primary author and the research and literature, manuscript content was contributed by both authors.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Evaluation of microneedling fractional radiofrequency device for treatment of acne scars. J Cutan Aesthet Surg. 2014;7:93-7.
- [CrossRef] [PubMed] [Google Scholar]
- Selective photothermolysis: Precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220:524-7.
- [CrossRef] [PubMed] [Google Scholar]
- 27.12 MHz radiofrequency ablation for benign cutaneous lesions. Biomed Res Int. 2016;2016:6016943.
- [CrossRef] [PubMed] [Google Scholar]




