
Translate this page into:
Simple Technique for Facial Dimple
Address for correspondence: Asst. Prof. Ahmed Hassan El-Sabbagh, Department of Plastic Surgery, Faculty of Medicine, Mansoura University, Mansoura, Egypt. E-mail: elsabbagh17@hotmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background:
Subjects seeking aesthetic surgery for facial dimples are increasing in number. Literature on dimple creation surgery are sparse. Various techniques have been used with their own merits and disadvantages.
Materials and Methods:
Facial dimples were created in 23 cases. All the subjects were females. Five cases were bilateral and the rest were unilateral.
Results:
Minor complications such as swelling and hematoma were observed in four cases. Infection occurred in two cases. Most of the subjects were satisfied with the results.
Conclusions:
Suturing technique is safe, reliable and an easily reproducible way to create facial dimple.
Level of Evidence:
IV: Case series.
Keywords
Facial dimple
suturing technique
closed technique

INTRODUCTION
Scars like umbilicus or deformities like chin and cheek dimples (small hollows) are established aesthetic features in plastic surgery. In Arabian society, cheek dimples are considered as a sign of beauty and attractiveness. The same concept is also established in oriental communities.[1]
Cheek dimples are caused by the presence of dermocutaneous insertion of the fibers of the inferior bundle of the double or bifid zygomaticus major muscle. Either or both of the cheeks can present with one or more dimples. Dimples occurring on both cheeks are more common than only one cheek.[2]
Several techniques had been described for creation of cheek dimples depending on two main principles either to excise soft tissue[3] or to use suturing technique.[45] In this article, suturing technique was used with some modifications.
MATERIALS AND METHODS
This study included 23 female subjects working at King Salman Hospital, Riyadh, Saudi Arabia, who underwent creation of 28 dimples (five cases were bilateral) during the period from August 2013 to August 2014. Informed consent was obtained from all individual participants included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Subjects were informed about the following: Swelling and oedema is likely during the first week. Mouth wash and fomentation (cold in the first 48 h and warm on the following three days) is advised. The dimple will be exaggerated in appearance and with time it will appear only with smiling (after one month) and within six months it will fade.
Operative technique [Video online Movies 1, 2]
The surgery was carried out as described by Bao and his colleagues[4] but with some modifications. The ideal location for marking of unilateral or bilateral dimples would be the area where a less obvious faint dimple is present with smiling. If a pre-existing dimple is not present, it is marked at the intersection of a perpendicular line dropped from the external canthus and a horizontal line drawn from the angle of the mouth.[1] Sometimes the marking migrated slightly laterally if pulsation of facial artery is palpable to avoid hematoma. The site of dimple may be at the level of angle of mouth or above it according to vector of smile.
The operation was performed with the subject under local anaesthesia [Figure 1]. The syringe with needle was introduced through the cheek from the marked skin and pulled from the site of puncture of the buccal mucosa. A 1-0 monofilament nylon or Prolene suture was inserted into the pinhole of the syringe needle and pumped from the hub of the syringe needle using the vacuum extractor side. After the suture had been pulled from the bottom of the syringe, the needle was gradually withdrawn from the dermis.
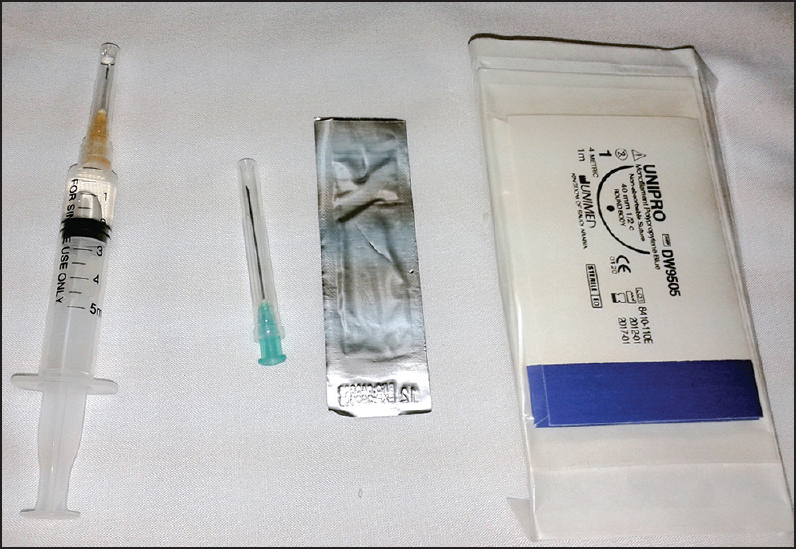
- Instruments used for the facial dimple surgery
The direction of the needle point was changed, punctured through the dermis and the muscle, and pulled to the buccal mucosa again at a different site (above the previous puncture in long face [Figures 2 and 4] and at the same level in round face [Figures 3 and 5].
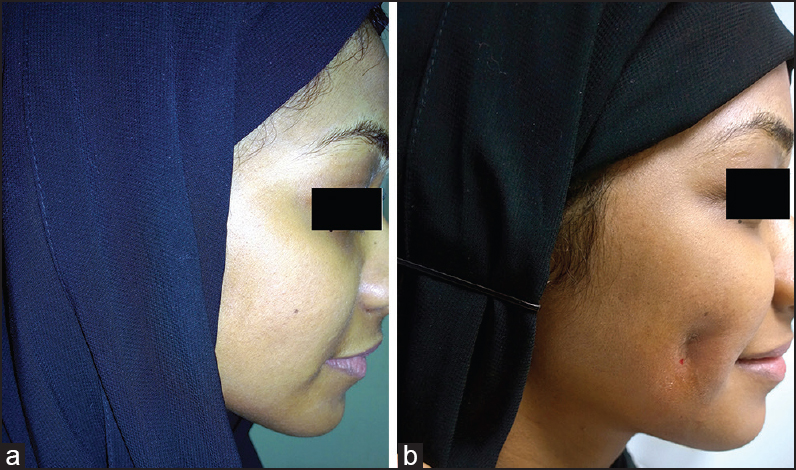
- Patient with long face with dimple on right side (a) pre (b) post

- Patient with round face with dimple on right side (a) pre (b) post
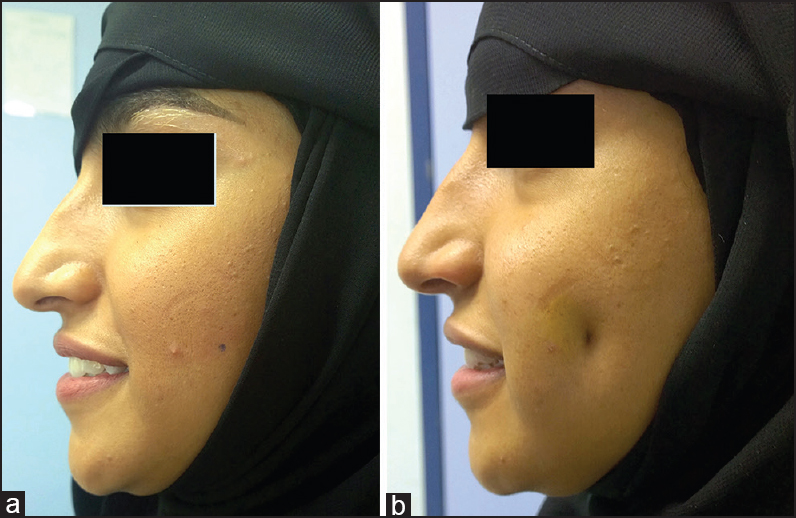
- Patient with long face with dimple on left side (a) pre (b) post

- Patient with round face with dimple on left side (a) pre (b) post
The suture was pulled from the pinhole of the syringe needle, and the syringe needle was removed from the skin. The active facial muscles and the dermis were sutured together. The knot is exaggeratedly tied, and the dimple was formed.
RESULTS
Twenty-eight dimples were created in 23 subjects. The subjects’ age ranged from 22 to 34 years. Five subjects requested bilateral dimples and 18 subjects requested single dimple mostly on the right side (12 cases right and six cases left).
The appearance of the dimple became more natural by the end of first week [Figures 2–5]. Postoperative infection occurred in two single dimple cases (done by Prolene suture). Infection was resolved by removal of suture, whereas three subjects had oedema and hematoma formation relieved by warm fomentation [Figure 6]. No subjects had injury to the Stensen duct or facial nerve branches. Sutures were removed after six weeks. There was no difference in results between subjects keeping sutures (six cases) and those who removed the sutures (15 cases). All dimples fade by the end of the sixth month. Three subjects requested to repeat the operation after fading and six subjects were seeking to add dimple on the other side. The procedure was repeated upon eight subject's request. Two subjects were dissatisfied with the appearance. Of the subjects, 15 have been followed up for six months.

- Redness and swelling dimple on right side
DISCUSSION
Beauty of the face is intimately related to expressions. A portrait of a beautiful face is never as beautiful as a face that is alive and expressive. The ultimate beauty of the face is augmented with the presence of dimples.
The presence of dimples is inherited in an autosomal dominant fashion. The cheek dimples are expressed on chromosome 16, with variable penetrance and ultimately parents with dimples will pass this to their children. There is increased demand for the creation of facial dimples, and many females seek cosmetic surgeons to achieve facial dimple.[3]
Since Boo-Chai[1] took the credit for creation of facial dimple in 1962, several authors had reported different techniques for connecting the active facial muscles to the dermis. In 1971, Argamaso[6] excised the cylindrical segment of tissue consisting of the buccal mucosa, muscle and subcutaneous fat to form a permanent dimple.
Many techniques have been introduced to create cheek dimples. They can be categorized into two major categories: Suturing with or without blind coring technique and open approaches.
Bao and his colleagues (2007) described an elegant technique where they used a syringe needle to guide a monofilament nylon suture through the dermis and the active facial muscles (usually the buccinator), a sling was formed between the skin and the buccinator muscle, the knot was tied, and the dimple was created.[4]
Keyhan and his colleagues (2012) said that for better suturing technique, the enhanced exposure is useful particularly in subjects with ‘chubby’ cheeks, where the depth of the field and fat tissue can make precise suturing difficult. The blind core procedure using a trephine bur was described. This approach provides a predictable outcome with persistence of dimple more than one year.[3]
Thomas et al. (2010) claimed that the anomalous anatomy responsible for dimples is surgically mimicked without requiring any soft tissue removal but by allowing adequate exposure.[5] Contrary to what was proposed, an incision in mucosa was done. Also, dissection of muscle with cutting part of buccinator muscle was made.
Indeed, open technique and blind core method have the same permanent results (up to 1 year). Suturing alone without excision of tissue has no lasting results and the dimple will fade with time.
In this work, Bao technique[4] was done with some refinements, where no incision in mucosa or absorbable sutures were performed. Marking was modified according to the location of facial artery pulsation to avoid hematoma formation. Regarding the shape of the face, the dimple was rounded or vertical. Also, the level created according to the vector of smile. Moreover, one suture was used instead of multiple sutures.
There was no standard scale used by all authors, the results vary and the outcome was different. Only, Argamaso evaluated his results using a scale including excellent, good, acceptable, not acceptable and failure.[6]
Most women hope that the side effects of the operation will be slight with short recovery period. Potential complications of dimple surgery include sudden disappearance of the dimple, asymmetry, foreign body reaction, bleeding, and nerve injury (buccal branch of the facial nerve) or salivary gland duct injury (Stensen duct), which are rare. Infection and oedema occurred with Prolene rather than nylon sutures. However, Prolene produced more lasting results. This may be due to more tissue reaction and fibrosis.
The open techniques that necessitate excision of tissue have got a risk of bleeding during or after dimple creation surgery. There is also an increased risk of haematoma formation and infection.
Advantages of using suture technique are less hematoma or infection. Other advantages of this technique include the following:
-
Mild postoperative swelling occurs and, consequently, subjects can return to work or other activities two days after the operation;
-
It is easy to adjust the bulk of dimples by adjusting the tension of the knot and the amount of dermis tissue; and
-
No tissue was excised.[4]
Also, this work has a reasonable follow up to six months and the dimple persists from three to four months. In addition, this study has an advantage that our technique was carried on in an average scale of subjects (23 subjects) done by a single surgeon. Moreover, this technique is very easy and fast as the surgical procedure time did not pass 90 s per side to create the dimple.
The main disadvantage of this technique is fading or complete disappearance after four months. In my opinion, permanent results after dimple creation are not an advantage. Personality of the subject (changing mind) or becoming dissatisfied with the appearance of dimple force the surgeon to find a solution for removal of dimple.
Authors from Australia advocated the use of medium-density hyaluronic acid fillers for resolving dimple formation.[7] Others used subcision with needle through subcuticular undermining with or without subcutaneous filler injection to fade the dimple.[8] With this technique, fading of dimple can be achieved by removal of sutures before six weeks or waiting for — four to six months. Many ancillary procedures such as Botox and injectables do not persist for more than six months.
In summary, all techniques described for creation of facial dimples are fruitful and reproducible, but becoming simple and conservative is the best way for better outcome.
CONCLUSION
Suturing is a simple and safe method for creation of cheek dimple whether for the subject or the surgeon. Consideration of vascular anatomy, shape of the face and smile direction are important aspects for the outcome.
Ethical standards
This study was performed in accordance with the ethical standards set forth in the 1964 Declaration of Helsinki and its later amendments.
Informed consent was obtained from all individual participants included in the study. Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.
Video available on www.jcasonline.com
Source of Support: Nil.
Conflict of Interest: I do not have any financial interests or commercial associations to disclose.
REFERENCES
- The facial dimple-clinical study and operative technique. Plast Reconstr Surg Transplant Bull. 1962;30:281-8.
- [Google Scholar]
- Double or bifid zygomaticus major muscle: Anatomy, incidence, and clinical correlation. Clin Anat. 1998;11:310-3.
- [Google Scholar]
- Dimple creation surgery technique: A review of the literature and technique note. J Oral Maxillofac Surg. 2012;70:e403-7.
- [Google Scholar]
- A new simple technique for making facial dimples. Aesthetic Plast Surg. 2007;31:380-3.
- [Google Scholar]
- Improved surgical access for facial dimple creation. Aesthet Surg J. 2010;30:798-801.
- [Google Scholar]
- Dynamic and static dimples: Early and late results. Aesthetic Plast Surg. 1981;5:173-82.
- [Google Scholar]
- Needle subcision: A conservative treatment for facial dimpling after elimination of odontogenic infection source: A technical note. Oral Maxillofac Surg. 2014;18:415-8.
- [Google Scholar]




