
Translate this page into:
Solitary cylindroma of tragus of the ear mimicking a keloid
Address for correspondence: Dr. Rupali Bavikar, C 505, Siciliaa, BT Kawde Road, Ghorpadi, Pune - 411 001, Maharashtra, India. E-mail: rupalibavikar@yahoo.co.uk
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cylindromas are very rare primitive sweat gland tumours differentiating towards eccrine or apocrine line. We present a case of cylindroma of tragus of external ear in a 50-year-old female. It was diagnosed clinically as keloid. After excision, histopathological and immunohistochemistry (IHC) studies confirmed diagnosis of solitary cylindroma.
Keywords
Cylindroma
histopathology
immunohistochemistry
keloid
tragus

INTRODUCTION
Cylindromas are benign skin adnexal tumours. They present as slow growing nodules on the trunk, scalp or face. They can be single or multiple. Multiple cylindromas form turban tumours in the autosomal dominant, Brooke Spiegler syndrome. We present a case of cylindroma of tragus of left ear, clinically diagnosed as keloid, due to its location and presentation. The case is presented on account of peculiar site of lesion which lead to diagnostic difficulty clinically.
CASE REPORT
A 50-year-old female presented with a small, hyperemic nodule measuring around 2 × 1 cm on tragus of left ear [Figure 1a]. The lesion was painless and slow growing over a period of 1 year. It was clinically diagnosed as keloid because of its location and presentation.
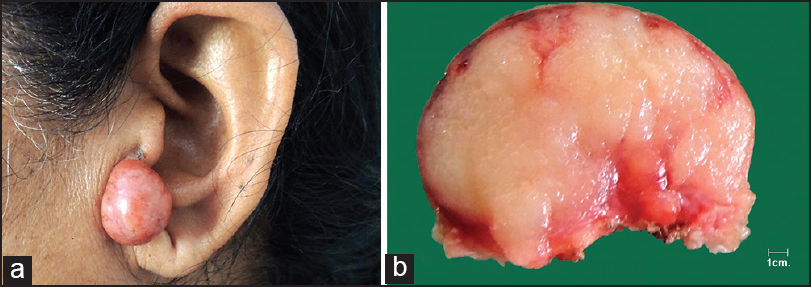
- (a) Covered reddish coloured lesion arising from tragus. (b) Cut surface of tumour showing greyish white lobular areas
Fine-needle aspiration (FNAC) of the lesion was done. The smears of FNAC showed small basaloid cells arranged around central hyaline globules. The cells were round to oval, monomorphic with bland nuclear chromatin [Figure 2a]. The differential diagnosis of basal cell adenoma and benign skin adnexal tumour was offered.
![(a) [400×, H and E] FNAC smear showing basaloid cells arranged around central hyaline amorphous material. (b) [100×, H and E] Islands of epithelial cells arranged like jigsaw puzzle and separated by hyaline sheath and a narrow band of collagen. Inset [400× H and E] showing two types of cells in island, cells with small dark staining nuclei and pallisading at periphery and cells with light staining large nuclei lie in the centre](/content/173/2015/8/2/img/JCAS-8-114-g002.png)
- (a) [400×, H and E] FNAC smear showing basaloid cells arranged around central hyaline amorphous material. (b) [100×, H and E] Islands of epithelial cells arranged like jigsaw puzzle and separated by hyaline sheath and a narrow band of collagen. Inset [400× H and E] showing two types of cells in island, cells with small dark staining nuclei and pallisading at periphery and cells with light staining large nuclei lie in the centre
Wide local excision of the lesion was done. On gross examination, it was a well-encapsulated, reddish brown coloured lesion. Cut surface was greyish white, lobular soft to firm [Figure 1b].
On microscopic examination, the lesion was located it the dermis. It was composed of cells arranged in nests and islands of round to oval cells arranged like a jigsaw puzzle and separated by eosinophilic hyaline basement membrane material. At the periphery, island of cells showed nuclear palisading and at places the cells were surrounded by hyaline material. At the centre of islands elongated myoepithelial cells were seen [Figure 2b]. Based on this a diagnosis of solitary cylindroma was entertained. Immunohistochemistry (IHC) markers were used to confirm the diagnosis. CK 7 (clone 5D7) was positive in basaloid cells [Figure 3a]. The peripheral hyaline basement material was stained positive for collagen IV (clone CIV22, Dako) [Figure 3b]. Smooth muscle actin (SMA clone 1A4, Dako) and S 100 were positive in myoepithelial cells. Based on histomorphological and IHC findings a diagnosis of solitary cylindroma of tragus was finalised.
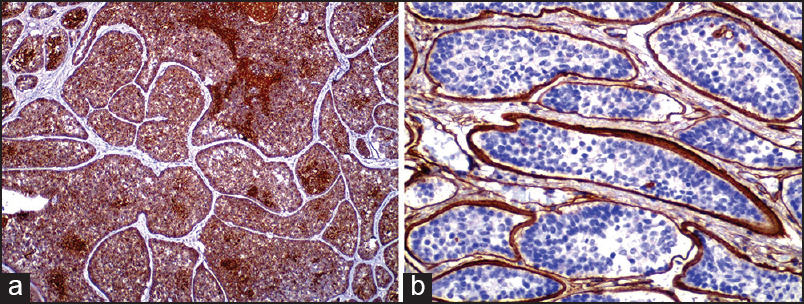
- (a) CK 7 was positive in central epithelial cells. (b) Collagen IV positivity in peripheral hyaline basement membrane material
DISCUSSION
Cylindromas are undifferentiated or poorly differentiated adnexal neoplasms of eccrine or apocrine lineage. They are small in size, solitary, slow growing lesions on the trunk, scalp or face. In our case, it was present on the tragus and mimicked a keloid.
Keloids are dermal fibrotic lesions considered as an aberration of the wound healing process. They are common after small skin excisions, ear piercing, drainage of auricular haematomas, repair of auricular traumas or as secondary keloid formations after prior keloid excision. Keloids are exophytic reddish purple smooth-surfaced lesions. In our case the lesion was located on the tragus and mimicked a keloid. Confirmed histopathological diagnosis of keloid vis à vis cylindroma is important as it impacts therapeutic management.[1]
The other differential diagnoses include: Auricular appendages and benign skin adnexal tumours like ceruminous adenoma and pleomorphic adenoma. Auricular appendages are harmless lesions, sometimes associated with Goldenhar syndrome and Wildervanck syndrome. Surgery is done for cosmetic purposes. Ceruminous adenoma and pleomorphic adenoma are benign tumours of cerumen secreting apocrine glands.[2] Histopathological examination is necessary for their diagnosis. Surgical excision is treatment of choice for these lesions.[3]
Cylindroma is a dermal tumour without attachment to the epidermis. It is composed of nests of tumour cells arranged in nested pattern. The nests are surrounded by PAS positive basement like material. The nests are composed of two cell types, peripheral cells are small basophilic with peripheral pallisading and larger, pale staining cells are seen centrally. Small tubular lumina filled with PAS positive material are seen in tumour nests.
Cylindroma can be single or multiple. A biopsy specimen is required for diagnosis.[4] Scalp cylindroma may present as multiple lesions, at times cover the entire scalp, labelled as turban tumour. Partial or complete hair loss usually occurs in these patients.[5] Multiple cylindroma are associated with Brooke-Spiegler syndrome, an autosomal dominant condition, with the CYLD gene on the chromosome 16q.[4] Although cylindromas are usually benign neoplasm, malignant transformation to cylindrocarcinomas is rare but well documented. Malignant cylindromas are locally aggressive and often metastasize.[56] Malignant cylindromas shows marked anaplasia and pleomorphism of nuclei. Abnormal mitotic figures are seen with invasion into the surrounding tissue.
For solitary lesions, the treatment of choice is surgical excision. Other treatments include electrodessication/curettage and cryotherapy. For small cylindromas, the carbon dioxide laser may be used.[7]
Multiple cylindromas usually require extensive plastic surgery that may be obviated by progressively excising a group of nodules in multiple procedures.
CONCLUSION
To conclude, cylindromas are benign skin adnexal tumour of eccrine or apocrine gland origin. They should be considered in differential diagnosis of lesions of external ear. IHC plays an important role in cases with diagnostic difficulty.
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- Efficacy of triple therapy in auricular keloids. J Cutan Aesthet Surg. 2014;7:98-102.
- [Google Scholar]
- Tumors arising from the glandular structures of the external auditory canal. Laryngoscope. 1983;93:326-40.
- [Google Scholar]
- McCalmont in Adnexal tumors. In: Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology (3rd ed). St Louis, MO: Mosby Elsevier; 2008. p. :1845.
- [Google Scholar]
- Brooke-Spiegler syndrome: Treatment with laser ablation. Clin Exp Dermatol. 2005;30:355-7.
- [Google Scholar]




