
Translate this page into:
Surgical pearl: Use of micropore tape for easy harvestation and transfer of suction blister epidermal graft
*Corresponding author: Muhammed Mukhtar, Department of Dermatology, Mukhtar Skin Centre, Katihar Medical College Road, Katihar, Bihar, India. drmmukhtar20@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mukhtar M. Surgical pearl: Use of micropore tape for easy harvestation and transfer of suction blister epidermal graft. J Cutan Aesthet Surg. 2025;18:61-2. doi: 10.25259/jcas_53_21
Abstract
Epidermal graft produced by suction is useful in treating vitiligo. However, it is very difficult to handle thin, flimsy, and translucent epidermis due to its in-curling and wrinkling properties. This is due to the hemispherical blister roof surface area which is twice its circular base. The correction of the epidermal surface and its resizing is a cumbersome and time-consuming task during epidermal grafting. To combat these problems, the blister roof is patched with micropore adhesive tape as a novel technique for harvestation and transfer of the suction blister graft.
Keywords
Diffuse pigmentation
Epidermis
Hemisphere
Incurling
Micropore
Mosquito artery forceps
Perifollicular pigmentation

PROBLEM STATEMENT
Epidermal graft produced by suction is useful in treating vitiligo. However, it is very difficult to handle a thin, flimsy, and translucent epidermis due to its in-curling and wrinkling properties like a deflated balloon. This is due to the hemispherical fibrinous blister roof, whose surface area is twice its circular base. The correction, identification of the epidermal surface, and its resizing are cumbersome and time-consuming tasks during epidermal grafting.1,2 To combat these problems, the blister roof is patched with micropore adhesive tape as a novel technique for harvestation and transfer of the suction blister graft.
RECOMMENDED SOLUTION
The blister roof is halved into two parts with the help of small scissors or a blade. The blister fluid is drained out. Subsequently, half of the graft is spread out well on its base to make it anti-curled and anti-wrinkled with the help of small mosquito forceps. Then, a piece of micropore tape is patched 1 on half of the graft. Following this, the mosquito forceps are inserted in the blister cavity to stretch out gently its margin, and then, the incised margin of the graft is held with the forceps to detach from its base completely [Figure 1a-d]. The same procedure was repeated to detach the second half of the graft. During the procedure, the tape was kept dry for better adhesiveness of the tape on the graft. The tape gives strength to the delicate graft and prevents the graft from getting torn. After harvestation, the epidermis remained uncurled and unwrinkled. This graft can be resized into any size and shape. There is no problem with surface identification, in-curling, and anti-wrinkling of the graft. The graft could be handled, transferred, or transported easily from the donor with the help of a forceps. Here, it is easily harvested, lifted, and re-grafted over the donor site. The taking of the graft does not interfere with the patching of tape which could be seen as the difference in the pattern of pigmentation (perifollicular vs. diffuse) without and with epidermal re-grafting over the donor site [Figure 2a and b]. Extra tape can be trimmed before grafting. There is no significant loss of graft on the margin and no incidence of secondary bacterial infection on a clean grafted wound.3

- (a-d) The different stages of harvestation of the first half of the graft.
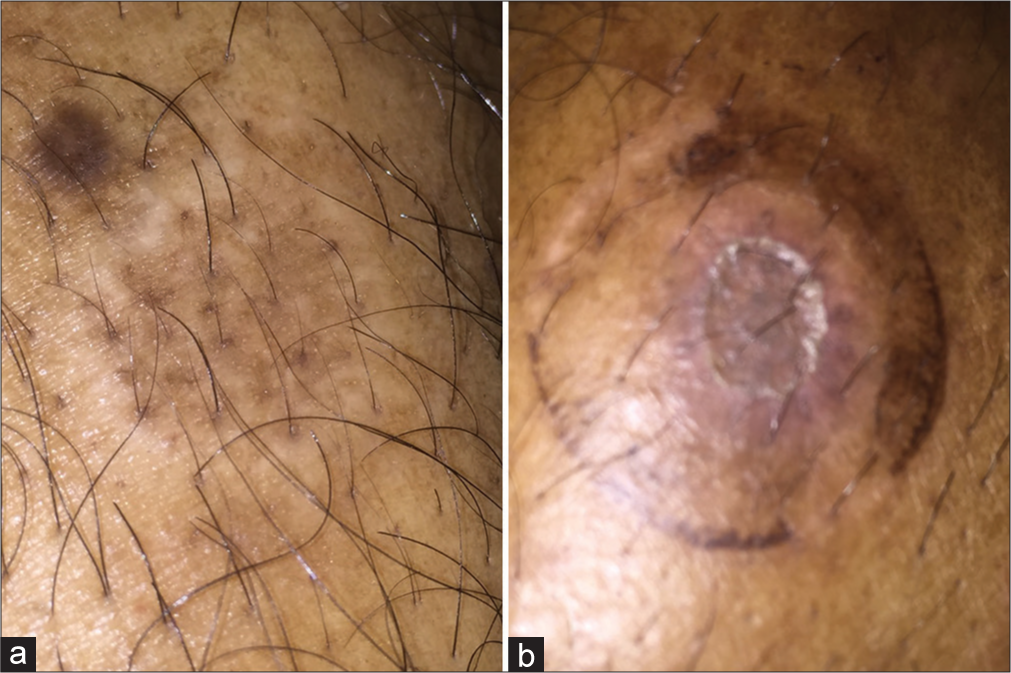
- (a) The pigmentation of donor sites without epidermal grafting showing patchy and perifollicular pigmentation and (b) diffuse pigmentation after epidermal grafting.
Authors’ contributions
All works related to this article are done by the author.
Ethical approval
Institutional Review Board Approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Resizing blister roof grafts for vitiligo surgery. J Am Acad Dermatol. 2014;71:e39-40.
- [CrossRef] [Google Scholar]
- Surgical pearl: Gloved finger as a transport platform for epidermal graft of suction blister. J Am Acad Dermatol. 2007;57:S118-9.
- [CrossRef] [Google Scholar]
- A retrospective comparison of 3M™ Micropore™ with other common dressings in cosmetic breast surgery. J Plast Reconstr Aesthet Surg. 2019;72:424-6.
- [CrossRef] [Google Scholar]




