
Translate this page into:
The Curious Case of Fibrofatty Conversion of Cystic Hygroma Treated with Bleomycin Sclerotherapy
Address for correspondence: Dr. Rohini Gupta Ghasi, Department of Radiodiagnosis, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi 110029, India. E-mail: rohini1912@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Cystic hygroma is a congenital malformation of the lymphatic system that mostly presents at birth. Though the classic treatment of this condition is surgical excision, recent alternative treatment modalities such as injection of sclerotherapeutic agents (e.g., bleomycin and OK-432) into the lesion has gained popularity due to its safe and effective response profile with minimal side effects. We report a rare complication of repeated bleomycin sclerotherapy in a follow-up patient of cystic hygroma, where the lesion underwent fibrolipomatous conversion with insinuation into multiple fascial planes, causing mass effect by encasement and compression of major vascular and airway structures. This is the first time such a complication of bleomycin sclerotherapy has been reported in literature. Such an unusual presentation reminds us that, in any patient presenting with recurrent gradually increasing swelling with worsening of symptoms following bleomycin sclerotherapy, a possibility of fibrolipomatous conversion of cystic hygroma should be borne in mind.
Keywords
Bleomycin
cystic hygroma
sclerotherapy

INTRODUCTION
Lymphangiomas are benign hamartomatous lymphatic tumors, which may occur anywhere in the body, though most frequently seen in neck (75%), axilla (20%), and inguinal areas (2%).[1] Cystic hygroma is the most common form of lymphangioma occurring in head and neck region.[2] Sclerotherapy with bleomycin is a favored treatment regime for cystic hygromas, with minimal side effects and good response rate.[2] Fibrolipomatous conversion of cystic hygroma after recurrent bleomycin sclerotherapy has hitherto been unreported in literature. We report an index case of such a complication, which led to worsening of symptoms in the patient.
CASE REPORT
A 26-year-old male patient presented with a large swelling on the left side of neck along with the complaints of difficulty in breathing and swallowing. The patient was a previously diagnosed case of congenital cystic hygroma [Figure 1], who had undergone surgical excision twice at the age of 6 months and 8 years, only to gradually develop recurrent swellings at the same site. These swellings were treated with bleomycin sclerotherapy every 3 years. However, patient had an apparent “non-response” to sclerotherapeutic agent such as bleomycin since past 4 years, and hence was referred to us for a contrast-enhanced computed tomography (CECT) to ascertain the cause of increasing size of swelling and worsening of symptoms. The clinical provisional diagnosis was a recurrence of cystic hygroma in the patient.
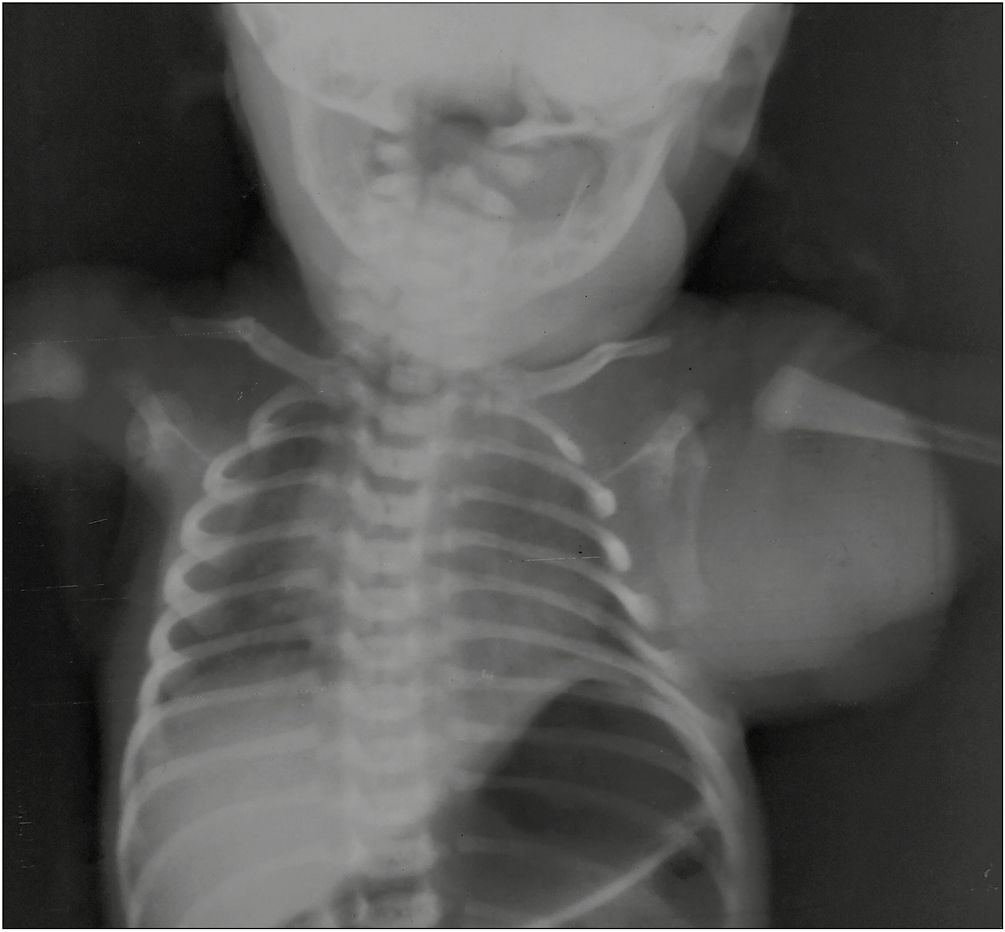
- Frontal radiograph of neck and chest of the patient as an infant shows soft tissue swelling along neck, shoulder, axilla, and chest wall on left side, diagnosed as congenital cystic hygroma
CECT of neck and thorax revealed a large non-encapsulated mass located in the left lateral aspect of neck and chest wall and left axilla [Figure 2]. The mass was a predominantly fat attenuation and contained few areas of coarsely calcified tubular soft tissue structures in the posterior aspect of neck and chest wall [Figure 3]. Few linear enhancing soft tissue components were also seen within the lesion.
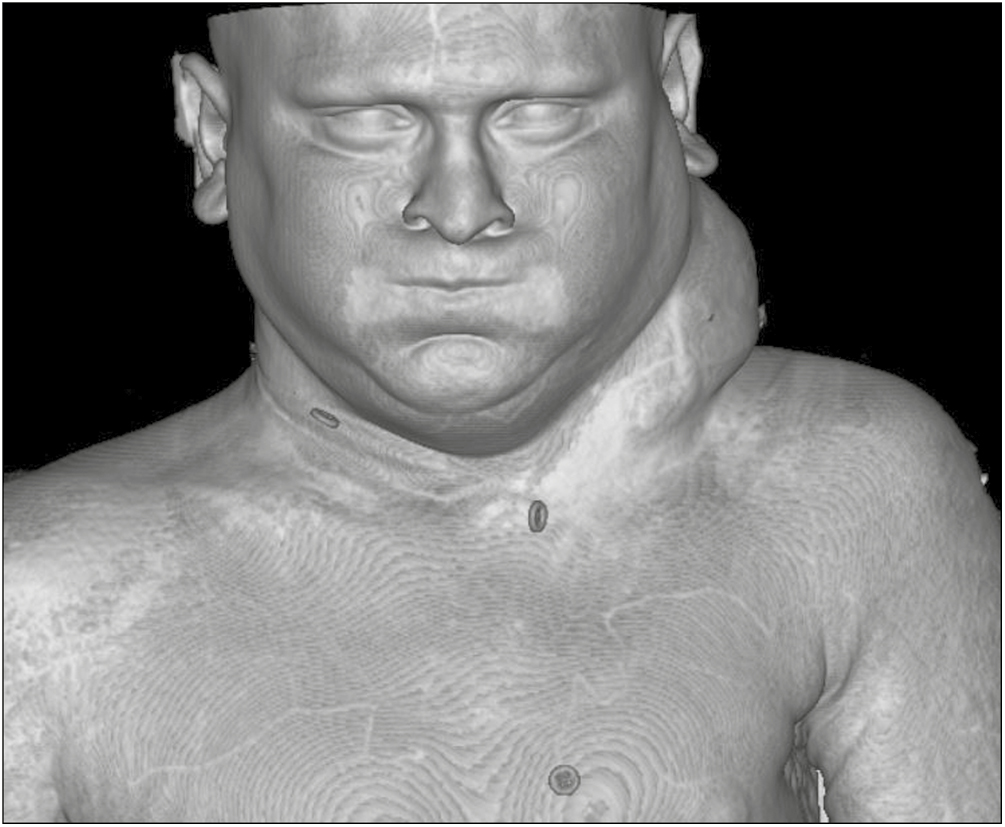
- Three-dimensional volume-rendered CT image of the patient shows a large swelling on the left side of neck and chest wall
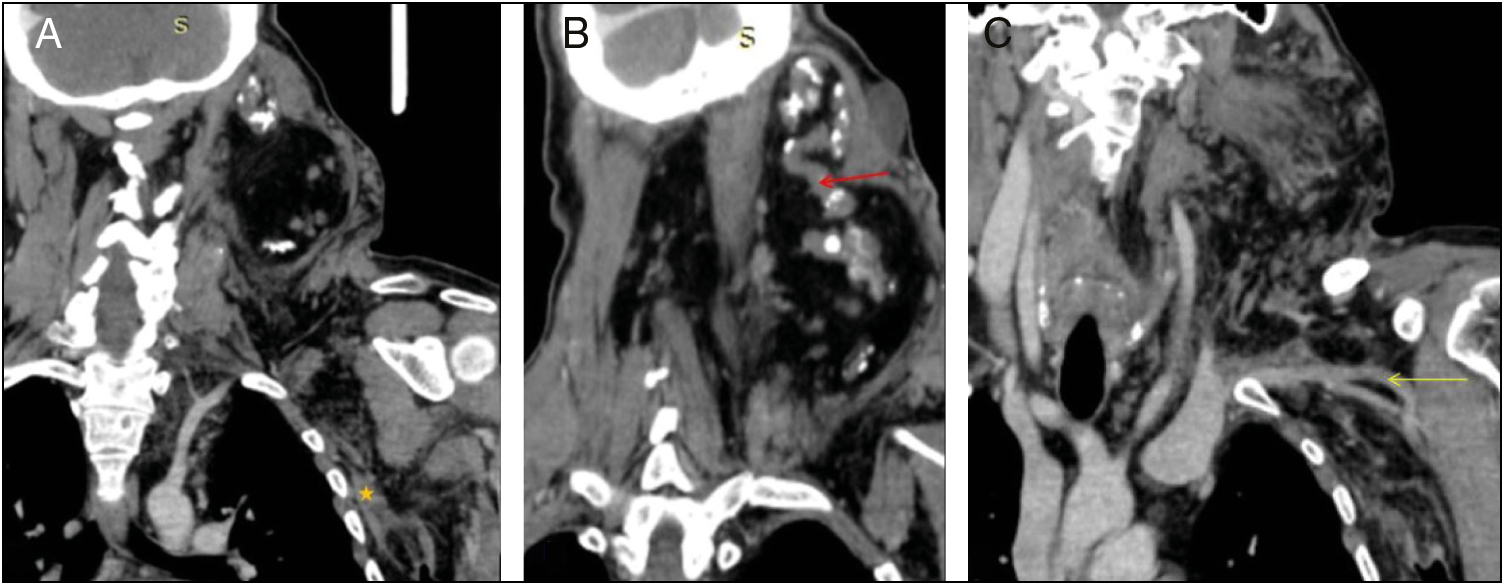
- CECT reveals a fatty mass in neck, chest wall, and axilla on left extending into superior mediastinum, with linear enhancing soft tissue components (asterisk) (A) and calcified tubular soft tissue structures (red arrow) (B) within. Lesion is also encasing left subclavian and axillary vessels (yellow arrow) (C) with fatty replacement of left sternocleidomastoid, trapezium, and scalene muscles
The lesion was diffusely infiltrative, and was seen extending from subcutaneous planes into inter- and intramuscular plane without respecting soft tissue planes, with subsequent fatty replacement of left sternocleidomastoid, trapezius, posterior paravertebral, and scalene muscles [Figure 3]. The lesion extended from scalp in left occipital region to D7 vertebral level along the posterior thoracic wall. No bony erosion was observed. Anteriorly, it reached up to the subcutaneous plane in neck and left anterior chest wall, abutting and narrowing left external jugular vein. Left axillary vessels were narrowed. Superomedially, lesion infiltrated into the floor of mouth, left supraglottis, and glottis, causing deviation of airway toward right side along with significant narrowing of airway and obliteration of left pyriform sinus [Figure 4]. Mass effect was present in the form of right-sided deviation of trachea, esophagus, and thyroid gland [Figure 4]. There was insinuation into superior mediastinum with encasement and narrowing of left internal jugular vein, left common carotid artery, and left subclavian artery. Considering the treatment history and imaging findings, a diagnosis of post-sclerotherapy fibrolipomatous conversion of cystic hygroma was made. The patient was planned for lipectomy in view of symptomatic airway compression.
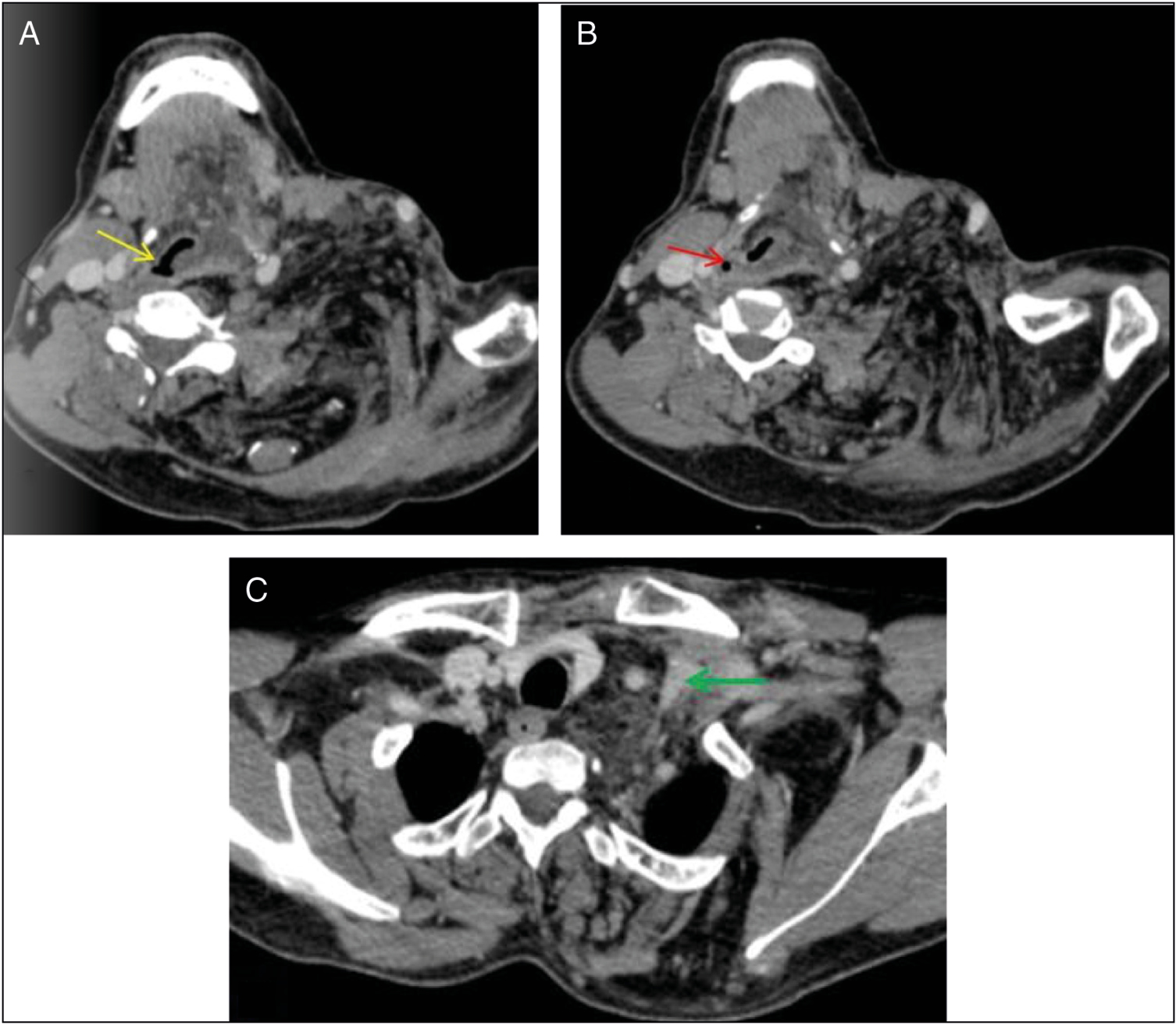
- Axial CECT sections depicting lesion infiltration into the floor of mouth, supraglottis (A, B), and glottis (C) on left, causing narrowing and right-sided deviation of airway (yellow arrow) with complete obliteration of left pyriform sinus. Right pyriform sinus is small but visualized (red arrow). There is right-sided deviation of trachea, esophagus, and thyroid gland by lesion with encasement of left common carotid artery and internal jugular vein (IJV), causing progressive narrowing and elongation of vein (green arrow) in contrast to normal right-sided IJV
DISCUSSION
Lymphangiomas are endothelium-lined spaces containing lymph, which can occur anywhere in the body, with the most common sites being head and neck.[3] Landing and Farber classified them into: (1) lymphangioma simplex, consisting of capillary-sized channels; (2) cavernous lymphangioma, comprising dilated lymphatic channels; and (3) cystic hygroma, consisting of multiple cysts with straw-colored fluid within.[3] Cystic hygroma usually presents as a painless congenital mass, which may be complicated with feeding and respiratory difficulty, fever, or sudden increase in size of lesion due to hemorrhage or infection.[2] Ultrasound is the primary imaging modality, which clearly demonstrates the cystic nature. They are mostly multilocular, containing septations of variable thickness.[2] Infected or hemorrhagic lesions may show fluid-fluid level. Both computed tomography (CT) and magnetic resonance imaging ascertain the extent of lesion and relations of the cyst with neurovascular bundle, especially before surgery.
Management of choice is surgical excision, however, the feasibility of complete excision of lesion is often questionable due to its infiltrative nature.[3] Chances of vital organ injuries, bleeding, infection, and scar formation are highly associated with surgery.[4] A recurrence rate of 15% is reported whenever residual tissue is left behind.[4] Safe and alternative treatment modalities such as sclerotherapy are now preferred, which can be performed in surgically inaccessible lesions also.[1] OK-432 and bleomycin are currently the most favored sclerotherapy agents for treating cystic hygroma.[5] In addition, cauterization, simple drainage or aspiration, radiofrequency ablation, and laser excision are being tried as an alternative to surgery or to reduce the pressure effect on respiratory and feeding passages.[2] Bleomycin is a deoxyribonucleic acid (DNA) synthesis inhibitor with sclerosing effect on endothelial cells due to inflammatory reaction.[6] According to a study by Kumar et al.,[1] response to bleomycin injection on clinical and Doppler assessment was found as excellent, good, or poor based on 100%, >50%, or <50% regression of lesion, respectively.
In a large systematic review of literature comparing sclerotherapy agents used in vascular malformation of head and neck by Horbach et al.,[7] the most common side effect following sclerotherapy injection was cellulitis and skin ulceration. Facial nerve palsy and skin necrosis were associated with ethanol and OK-432 sclerotherapy. Mean complication rate of bleomycin therapy was 6% in their study, with skin infection, pain, and swelling being common adverse reactions. In another retrospective review by Alomari et al.,[8] no serious side effect was encountered in patients on bleomycin sclerotherapy. Chen et al.[9] observed that high doses of bleomycin injection could lead to pulmonary fibrosis, especially when total cumulative dose exceeds 400 mg. However, to the best of our knowledge, fibrofatty conversion of cystic hygroma, after bleomycin injection, has never been reported in literature before.
Another condition that simulates the CECT picture as seen in our case is Madelung’s disease, an idiopathic disease where non-encapsulated fat masses are deposited in the face and cervical region.[10] Surgical treatment of Madelung’s disease includes lipectomy and liposuction, especially to remove the mass effect on vital organs.[10] Use of steroids and antiretroviral drugs, which may cause fat deposition, was excluded in our patient.[8] Hence, in any case of suspected non-response to bleomycin sclerotherapy in cystic hygroma or paradoxical increase in size of lesion or symptoms, the possibility of bleomycin-induced fibrofatty conversion of cystic hygroma should be kept in mind and the patient should undergo imaging for evaluation of the same.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Intralesional bleomycin in lymphangioma: an effective and safe non-operative modality of treatment. J Cutan Aesthet Surg. 2012;5:133-6.
- [Google Scholar]
- Treatment of cystic hygroma by intralesional bleomycin injection: experience in 70 patients. Eur J Pediatr Surg. 2010;20:178-82.
- [Google Scholar]
- A unified concept of lymphangioma and cystic hygroma. Surg Gynecol Obstet. 1965;120:79-86.
- [Google Scholar]
- Intralesional bleomycin injection (IBI) treatment for haemangiomas and congenital vascular malformations. Pediatr Surg Int. 2004;19:766-73.
- [Google Scholar]
- Injection of bleomycin as a primary therapy of cystic lymphangioma. J Pediatr Surg. 1992;27:440-3.
- [Google Scholar]
- Sclerotherapy for low-flow vascular malformations of the head and neck: a systematic review of sclerosing agents. J Plast Reconstr Aesthet Surg. 2016;69:295-304.
- [Google Scholar]
- Percutaneous sclerotherapy for lymphatic malformations: a retrospective analysis of patient-evaluated improvement. J Vasc Interv Radiol. 2006;17:1639-48.
- [Google Scholar]
- Percutaneous sclerotherapy of massive macrocystic lymphatic malformations of the face and neck using fibrin glue with Ok-432 and bleomycin. Int J Oral Maxillofac Surg. 2011;40:572-6.
- [Google Scholar]
- Madelung’s disease: a benign symmetric lipomatosis. Indian J Dermatol Venereol Leprol. 2018;84:190-1.
- [Google Scholar]




