
Translate this page into:
Trypsinized suction blister
*Corresponding author: Suman Patra, Department of Dermatology, Venereology and Leprology, All India Institute of Medical Sciences Jodhpur, Rajasthan, India. patrohere@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Patra S, Kumar S, Kaur M. Trypsinized suction blister. J Cutan Aesthet Surg. 2025;18:56-7. doi: 10.25259/jcas_2_24
Abstract
Suction blister epidermal grafting (SBEG) is a standard technique for treating vitiligo on challenging areas like fingertips and lips but often results in pigment halos and difficulties with small, curved surfaces. We propose a modified SBEG technique, utilizing trypsinization of one blister graft to improve melanocyte spread and reduce peri-graft halo. Trypsin ethylenediaminetetraacetic acid (EDTA) solution is introduced into a selected blister, creating a cell suspension applied to dermabraded gaps and peripheries, including eyelid margins. At 5-month follow-up, complete re-pigmentation with no halo effect was achieved, indicating this modified approach’s potential in enhancing SBEG outcomes for complex sites.
Keywords
Perigraft halo
Suction blister grafting
Trypsinized modification of suction blister grafting

PROBLEM STATEMENT
Suction blister epidermal grafting is a well-established surgical technique for vitiligo.1 It is preferred over cellular grafts for fingertip and lip lesions due to its ease to perform over rounded and uneven surfaces. Its main limitation remains lack of spread of the engrafted melanocytes leading to halo around each graft. It has difficulty in re-pigmenting the eyelid margins and angle of mouth due to size of the graft and difficulty to apply it over small, curved surfaces.2
RECOMMENDED SOLUTION
We propose a modification of suction blister epidermal graft (SBEG) by trypsinization of one of the blister grafts to overcome the obstacle of pigment spread and minimize peri graft halo.
One of the blisters made for SBEG is chosen and blister fluid is aspirated through an 1 cc syringe attached to a 26G needle puncturing the blister through its floor. Equal amount of trypsin ethylenediaminetetraacetic acid (EDTA) solution is injected into the blister by the same needle and kept for 25–30 min. Then, the trypsin EDTA solution is aspirated completely. The graft is obtained by harvesting the roof of the blister over a glass slide. Apart from the blister graft, turbid fluid also comes out from the dermal side of the blister graft containing cell suspension [Video 1]. Over the dermabraded recipient area following application of rest of the blister grafts, the cell suspension is applied over the gaps between the grafts and also over the periphery (including the eyelid margin in our case). Dressing and subsequent care are similar to SBEG procedures. Complete re-pigmentation was achieved over the lesion including eyelid margin at 5th-month follow-up with no peri-graft halo [Figure 1a and b].
Video 1:
Video 1:Technique of trypsinized suction blister grafting.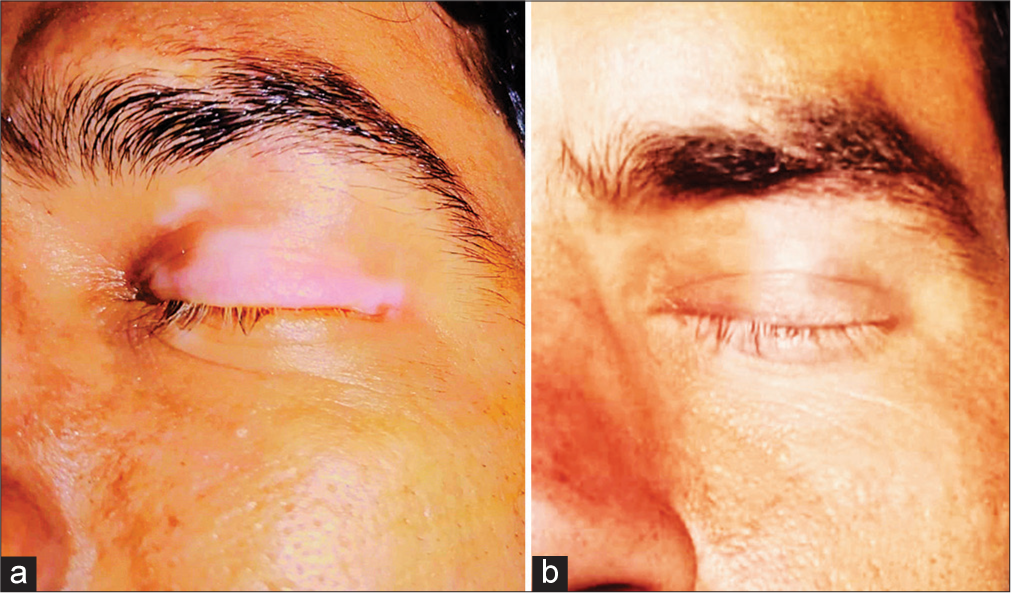
- (a) Pre-treatment photograph of the vitiligo lesion over upper eyelid, (b) post-treatment photograph after 5 months with complete repigmentation including the eyelid margin.
Authors’ contributions
All authors contributed equally during the process of surgery and drafting the same for publication.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Video available on:
Financial support and sponsorship: Nil.
References
- Suction blister grafting for vitiligo: Efficacy and clinical predictive factors. Dermatol Surg. 2015;41:633-9.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison between autologous noncultured epidermal cell suspension and suction blister epidermal grafting in stable vitiligo: A randomized study. Br J Dermatol. 2012;167:1295-301.
- [CrossRef] [PubMed] [Google Scholar]




