
Translate this page into:
Unusual Presentation of Trichoblastoma
Address for correspondence: Dr. C. Shanmuga Sekar, Department of Dermatology, PSG Institute of Medical Sciences and Research, Coimbatore 641 004, Tamil Nadu, India. E-mail: drshanmugasekar@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
We report a 39-year-old man who presented with skin-colored plaque over the glabella and root of the nose. Histopathology revealed the diagnosis of trichoblastoma. This case is reported to emphasize the rare presentation of trichoblastoma as it usually presents as an isolated nodule.
Keywords
Adnexal tumors
trichoblastoma
unusual presentation

INTRODUCTION
Trichoblastoma is a small benign hair follicle tumor originating from follicular germinative cells. It is thought to be a variant of trichoepithelioma. It typically presents as a solitary mass of small skin-colored to brown or blue-black papules or nodules, usually 1–2 cm in diameter.[1] They most commonly occur on the face, scalp, thighs, and perianal region of adults around 40–50 years of age.[2]
CASE REPORT
A 39-year old man presented with asymptomatic, skin-colored, raised lesions over the glabellar region for 2 years duration which gradually increased in size. On examination, skin-colored corrugated plaque over the glabella and root of the nose which was extending bilaterally over and above the eyebrows were present [Figure 1A]. Histopathology showed neoplasm composed of basaloid cells arranged in nodules, racemiform, reticulated, and cribriform patterns. Cells had bland nuclei and indistinct cell borders with palisading of nuclei. Nodules of follicular germinative epithelium composed of germ-like structure with peripheral palisading and surrounded by delicate fibrillary stroma were seen. Follicular differentiation of hair shafts and calcification was observed [Figure 2A–C]. There was no evidence of peritumoral retraction artifact. Immunohistochemical markers showed: Bcl 2 positivity for tumor cell population at the periphery, CD 10 positivity for stromal cells, CK 20 negativity, and Ki67 indicates low proliferative index – 10–15% [Figure 3A–D].
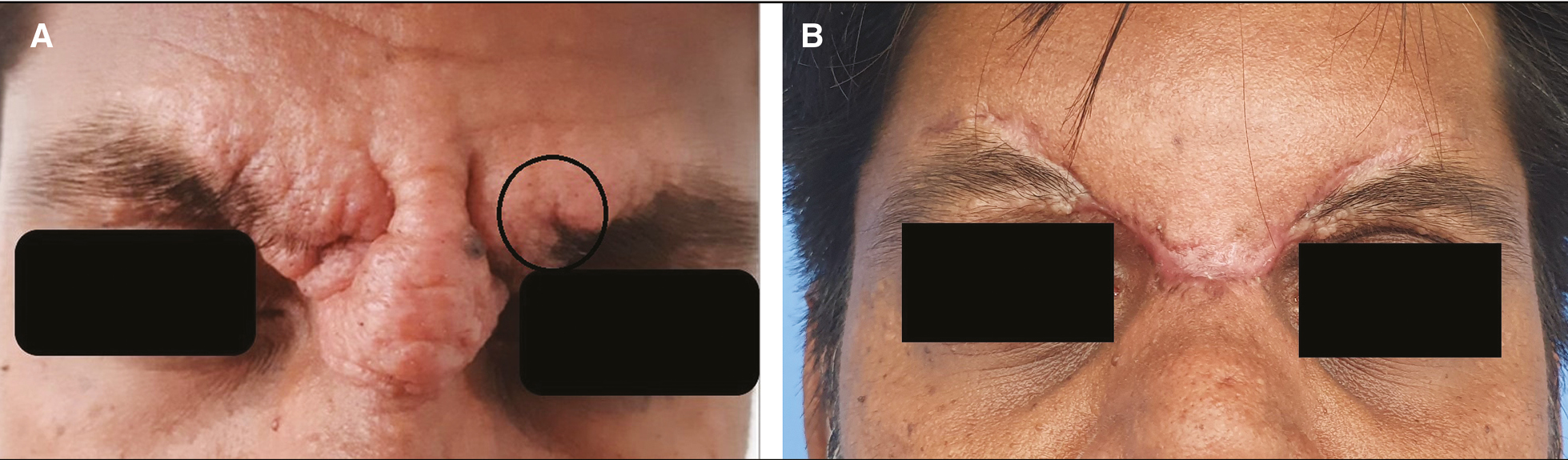
- (A) Skin-colored corrugated plaque over glabella and root of nose which were extending bilaterally over and above the eyebrows were present. (B) Postsurgical follow-up.
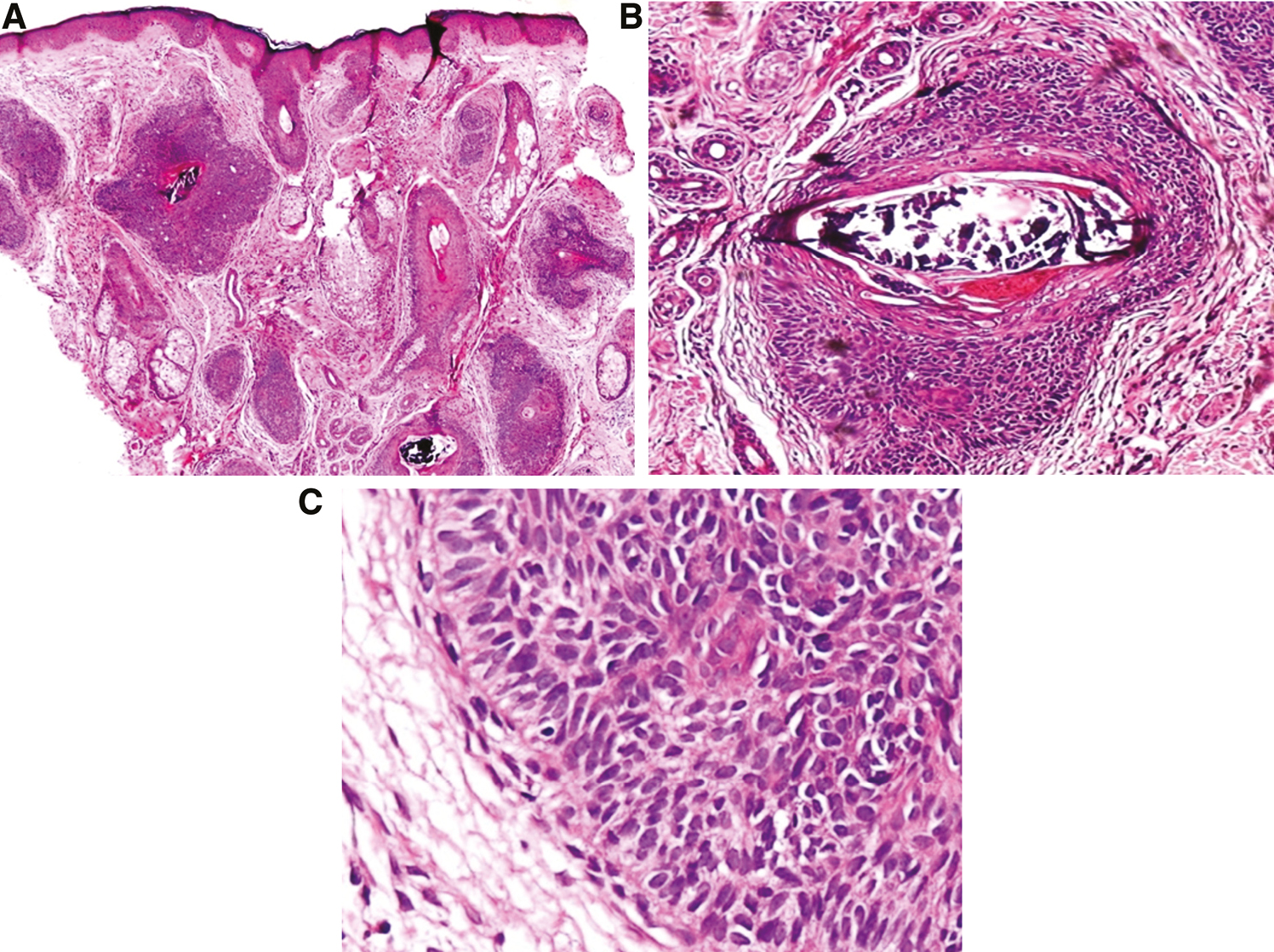
- (A) Atrophic epidermis. Dermis showed basaloid cells arranged in nodules (H&E, 40x). (B) Nodules of follicular germinative epithelium composed of germ-like structure with calcification at the center, surrounded by delicate fibrillary stroma (H&E, 100x). (C) Cells with hyperchromatic nuclei, scanty cytoplasm, and indistinct cell border with peripheral palisading (H&E, 400x).
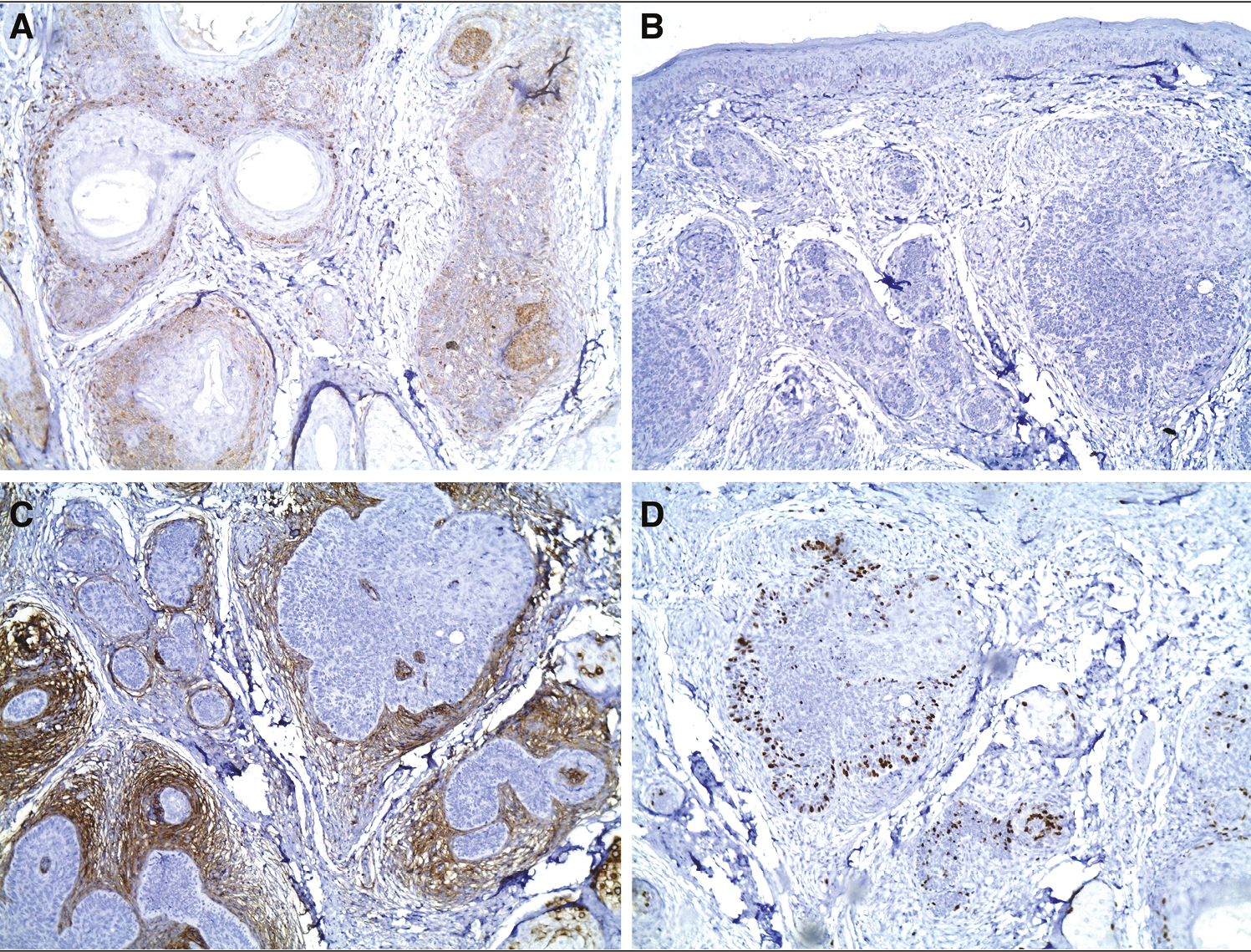
- Immunohistochemistry: (A) Bcl-2 cells at the peripheral show Bcl-2 staining (IHC, 40x). (B) Tumor cells are negative for CK-20 (IHC, 100x). (C) Stromal expression of CD 10 (IHC, 100x). (D) Ki-67 shows low proliferation index (IHC, 100x).
Based on clinical findings, histopathologic findings, and immunologic markers, diagnosis of trichoblastoma was performed.
We did CO2 laser ablation for a smaller area which responded well. Because the lesion was larger in size, we referred the patient to a plastic surgeon, and surgical excision with grafting was done [Figure 1B].
DISCUSSION
Trichoblastoma, a distinct variant of trichoepithelioma, is a small benign hair follicle tumor originating from follicular germinative cells. It typically presents as a solitary mass of small skin-colored to brown papules or nodules, usually 1–2 cm in diameter, predominantly in the head and neck area. The main difference between trichoblastomas and trichoepitheliomas is the depth at which they arise in the dermis. Trichoblastomas are found in the deep dermis and subcutaneous tissue, whereas trichoepitheliomas are more superficial.
Histopathologically, all trichoblastomas and trichoepitheliomas are linked by a predominance of follicular germinative (basaloid) cells with enveloping fibrocystic stroma that varies in degree.[3]
In 1970, Headington described the first case of trichoblastoma as a kind of benign skin neoplasm showing differentiation toward hair structures and he classified “trichogenic tumors” into four types are as follows: trichoblastoma, trichoblastic fibroma, trichogenic trichoblastoma, and trichogenic myxoma.[4] Usually, most trichoblastomas develop along only one line of differentiation (i.e., toward primitive hair follicles). Rare cases of trichoblastoma show multiple paths of differentiation toward more than one type of adnexal structure. Trichoblastomas can be divided depending on their clinical aspect (plaque-like, small nodular, and large nodular [giant] trichogenic tumors). Presentation varies from superficial plaques to papular or nodular lesions.[5]
Ackerman later classified trichoblastoma into five histopathologic patterns such as large nodular (including pigmented), small nodular, cribriform, racemiform, and retiform types. The latest classification includes subcutaneous, pigmented, clear cell, sebaceous, and sweat gland differentiation.
Histologically, trichoblastoma is a well-circumscribed, nodular tumor spanning the entire dermis, characteristically extending into the subcutaneous tissue. A purely subcutaneous location may be rarely seen. It is characterized by variable-sized epithelial nests, conspicuous peripheral palisading, and stromal condensation around the tumor lobules closely resembling basal cell carcinoma.[6]
The histologic findings in the plaque variant of trichoblastic fibroma may cause confusion with basal cell carcinoma because of its poor circumscription, deep extension, and mitotic rate. Identification of the mixed epithelial–mesenchymal components, analogous to the classic trichoblastic fibroma, should suggest the diagnosis. The key histologic features again include frondlike or anastomosing tumor islands, papillary mesenchymal bodies, and cellular, fibroblastic stroma. The previously unrecognized plaque variant is also slow-growing and may become quite large with ill-defined tumor margins. This variant may demonstrate locally aggressive behavior with an infiltrative growth pattern. Surgical excision appears to be an appropriate and prudent treatment, as these lesions may have a slow, but persistent, growth and attain a considerable size.[3]
CONCLUSION
This case presented as a corrugated plaque over glabella, a rarer presentation of trichoblastoma as it usually presents as an isolated nodule. We report this case for its clinical rarity.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Trichoblastic fibroma: Hair germ (trichogenic) tumours revisited. Histopathology. 1987;11:327-31.
- [Google Scholar]
- Benign trichogenic tumours: A report of two cases supporting a simplified nomenclature. Histopathology. 1993;22:575-80.
- [Google Scholar]
- Trichoblastic fibroma. A series of 10 cases with report of a new plaque variant. Arch Dermatol. 1995;131:198-201.
- [Google Scholar]
- Vulvar trichogenic tumors: A comparative study with vulvar basal cell carcinoma. Am J Surg Pathol. 2005;29:479-84.
- [Google Scholar]
- Melanotrichoblastoma: Immunohistochemical study of a variant of pigmented trichoblastoma. Am J Dermatopathol. 2002;24:498-501.
- [Google Scholar]




