
Translate this page into:
Use of a ticket punch and adhesive transparent dressings for injecting botulinum toxin in hyperhidrosis

*Corresponding author: Mihika Faye Noronha, Department of Dermatology, Joshi Hospital, Pune, Maharashtra, India. mihikanoronha@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mutalik SD, Noronha MF. Use of a ticket punch and adhesive transparent dressings for injecting botulinum toxin in hyperhidrosis. J Cutan Aesthet Surg. doi: 10.25259/jcas_33_24
Abstract
This article describes a novel modification in marking the sites of botulinum toxin injection in patients with axillary hyperhidrosis using a ticket punch and an adhesive occlusive sticker.
Keywords
Hyperhidrosis
Botulinum toxin A
Ticket punch
Innovation

PROBLEM STATEMENT
Marking multiple points for infiltration for administration of botulinum toxin hyperhidrosis is difficult along the axillary curvature. This method circumvents the need for sterile tapes and markers as the self-adhesive tape is provided along with topical anesthesia.
RECOMMENDED SOLUTION
Axillary hyperhidrosis is treated by injecting 50 units of botulinum toxin A into each axilla. Botulinum toxin is reconstituted with normal saline to reach a concentration of 20 units/mL. It is injected at a distance of 1–2 cm distance.1 These points are marked by marking points with a pen and ruler or drawing vertical and horizontal lines a centimeter apart to form a grid and injecting them at the intersection.2,3 This technique is tedious for the surgeon. Marking the injection points on transparent dressings overcomes this issue.1 However, this tends to blunt the needle, making the injections more painful. The area of hyperhidrosis was identified by the starch iodide test. Adhesive tape for occlusion often comes complementary with the eutectic mixture of local anesthesia that we use to numb the area. We have used a ticket punch [Figure 1] to punch holes at a 1–2 cm distance over a sheet of adhesive tape meant for occlusion that would cover the affected area [Figure 2]. The holes form a grid. The backing is removed and the adhesive tape is then pasted over the cleaned field of injection [Figure 3]. The botulinum toxin is then injected through the center of each hole. This simplifies the process as it is easier to mark along a flat plane of the adhesive as compared to the curvature of the underarm. There is less blunting of the needle with injecting through pre-punched holes compared to injecting through a grid marked on an intact dressing.

- Ticket punch.
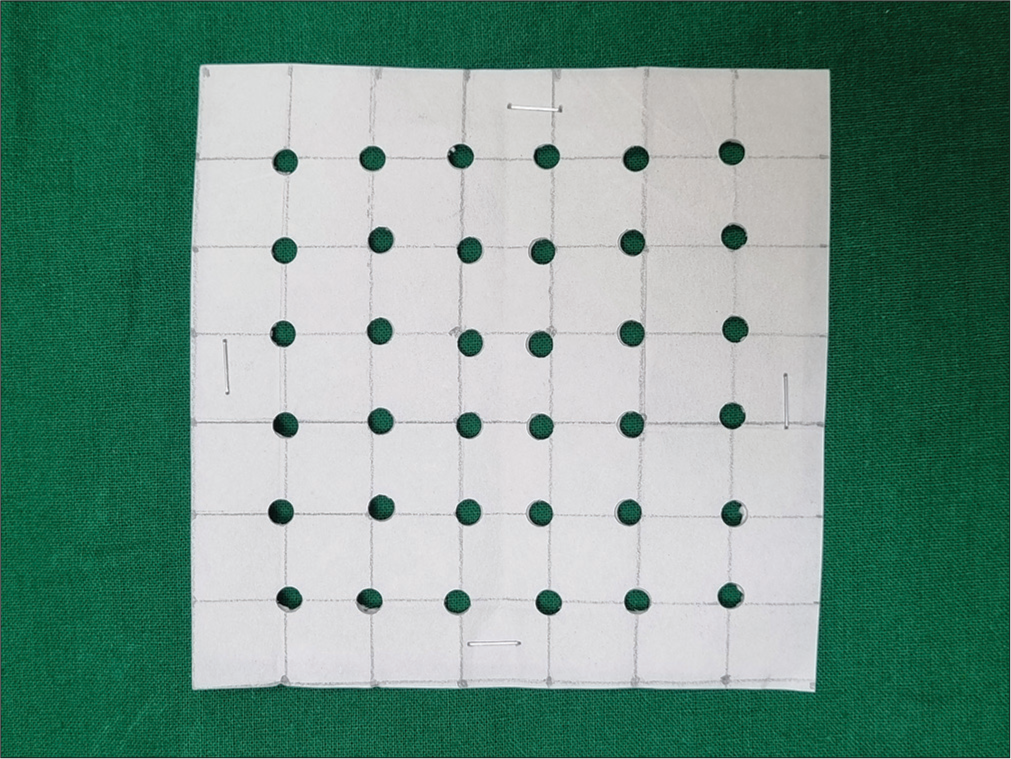
- Adhesive dressing punched in a grid.

- Adhesive on the skin.
Authors’ contributions
Sharad Mutalik contributed to the design and implementation of the research, Sharad Mutalik and Mihika Noronha to the analysis of the results and to the writing of the manuscript.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Botulinum toxin injection technique for axillary hyperhidrosis. Acta Dermosifiliogr. 2014;105:517-8.
- [CrossRef] [Google Scholar]
- A new multiple site marking grid for botulinum toxin application in the treatment of axillary hyperhidrosis. Br J Dermatol. 2006;154:385-6.
- [CrossRef] [Google Scholar]
- Severe primary axillary hyperhidrosis - dosing and administration-Botox one- BOTOX® (onabotulinumtoxina)®. Available from: https://www.botoxone.com/hyperhidrosis/dosing [Last accessed on 2024 Jan 25]
- [Google Scholar]




