
Translate this page into:
Treatment of the Ageing Hand with Dermal Fillers
Address for correspondence: Dr. Ulrich Kühne, Aesthetische Dermatologie im Medico Palais, Parkstraβe 6, D-65812, Bad Soden, Germany. E-mail: info@aesthetische-dermatologie.eu
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Following the trend in facial cosmetic procedures, patients are now increasingly requesting hand rejuvenation treatments. Intrinsic ageing of the hands is characterized by loss of dermal elasticity and atrophy of the subcutaneous tissue. Thus, veins, tendons and bony structures become apparent. Among the available procedures, intrinsic ageing of the hands is best improved by restoring the volume of soft tissue. Volume restoration can be achieved with a number of long-lasting dermal fillers with varying degrees of improvement and treatment longevity. The dermal fillers used in hand rejuvenation include autologous fat, collagen, hyaluronic acid, calcium hydroxylapatite and poly-L-lactic acid. Here, we describe our preferred injection method for hand rejuvenation using calcium hydroxylapatite and a single-bolus injection.
Keywords
Calcium hydroxyapatite
dermal fillers
fat grafting
hand rejuvenation
hyaluronic acid
poly-L-lactic acid

INTRODUCTION
Apart from the face and neck, the hand is the most visible unclothed area of the body.[12] However, despite great advances in facial cosmetic procedures, hand rejuvenation has been largely neglected.[23] Cosmetic patients notice that the aged appearance of their hands contrasts with their rejuvenated face,[13] and increasingly request hand rejuvenation procedures.[4]
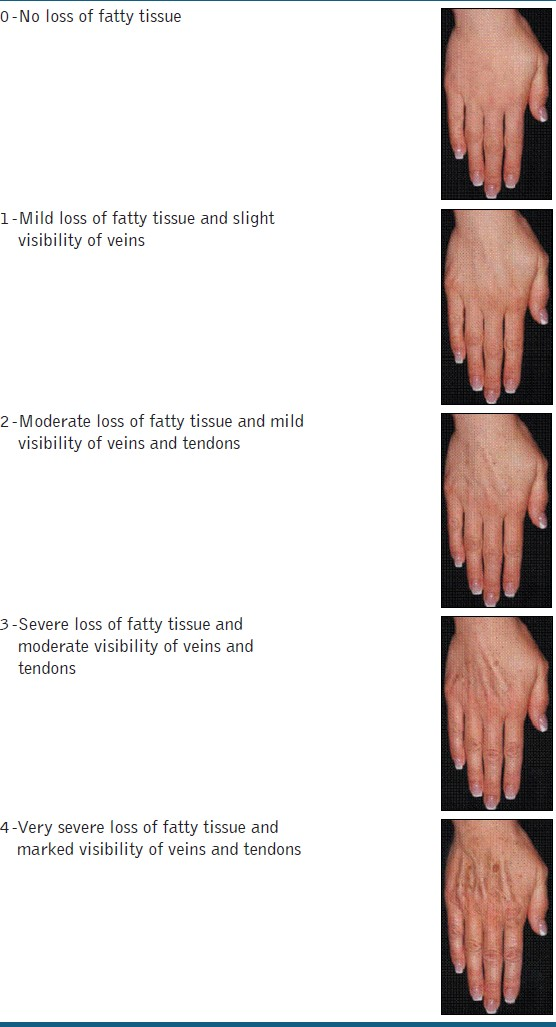
With age, the appearance of the hand changes, as illustrated in the 5-point Hand Grading Scale [Table 1],[5] due to both intrinsic and extrinsic factors.[4] Extrinsic ageing affects the epidermal and dermal layers following exposure to the sun, chemicals and smoking, and can manifest as actinic keratosis (premalignant), solar lentigines, punctate hypopigmentation and solar purpura.[34] In contrast, intrinsic ageing alters the deeper soft tissue planes, decreasing skin elasticity, soft tissue volume (dermal and fat atrophy) and dermal vascularity.[46] Signs of intrinsic ageing include wrinkles, translucent, lax and thinner skin and prominent veins, joints and tendons.[236]
A number of options are available to restore the youthful appearance of the hands. Most hand rejuvenation treatments focus on extrinsic ageing by unifying pigmentation and skin resurfacing. These treatments, including topical acids (tretinoin and vitamin C, among others), topical 5-fluorouracil, bleaching agents, microdermabrasion, chemical peeling (light and medium peels) and laser or intense pulse light treatments, have been shown to be the most appropriate.[34] However, some of these temporary treatments can be associated with permanent pigmentation changes and hypertrophic scarring.[12] Sclerotherapy and phlebectomy have been used to minimize the appearance of veins,[34] but these are uncommon procedures that can be unnecessary following volume restoration.[1] Hand volume restoration or contouring can address most intrinsic signs of ageing and can be used alone or in combination with other hand rejuvenation methods previously mentioned.[1] Here, we summarize the different dermal fillers used to restore the youthful appearance of hands and describe our preferred method of injecting calcium hydroxylapatite (CaHA; Radiesse®, Merz Pharmaceuticals GmbH, Frankfurt, Germany) for hand rejuvenation.
DERMAL FILLERS USED FOR HAND VOLUME RESTORATION
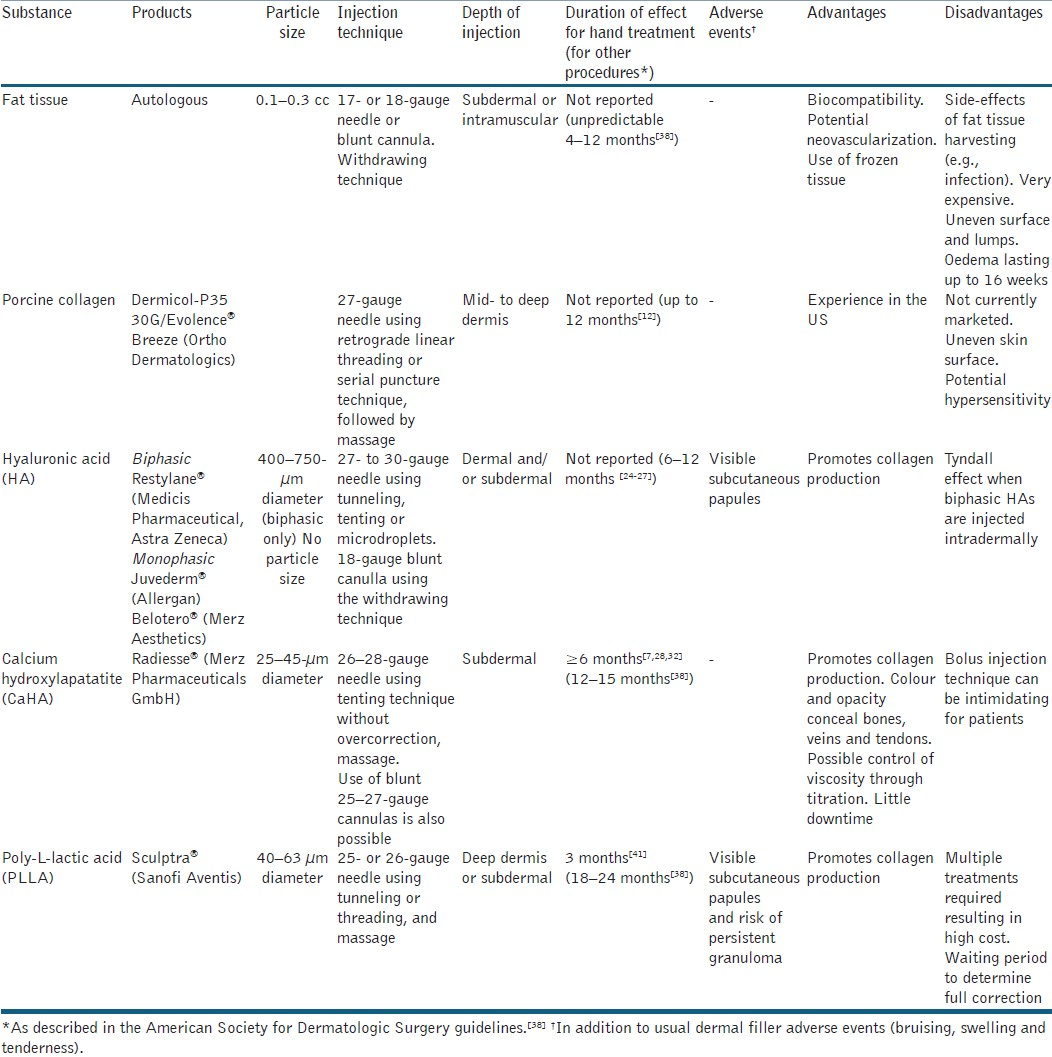
Volume restoration has been shown to improve skin elasticity and reduce the appearance of wrinkles and prominent structures in the ageing hand.[17] In cosmetic surgery, several dermal fillers have been developed, but long-lasting fillers are best adapted for volume replacement in the hand [Table 2].[78]
AUTOLOGOUS FAT INJECTION
Volume replacement with autologous fat has been successfully used in hands.[23] The method involves two steps, fat harvesting and fat injections. Fat harvesting, generally from the abdomen or upper thighs, is an invasive procedure with potential risk of infection, bruising and scarring.[1279] Fresh fat tissue, or previously harvested fat tissue that has been frozen and thawed, is then injected into the hands of patients.[3] Fat that has been centrifuged prior to injection has been associated with better results.[3] Multiple treatments are generally required and duration of effect is unpredictable, particularly with fat tissue that has not been centrifuged.[1310] An uneven surface and the presence of lumps have been reported in some patients, but this could be reduced by injecting small volumes of fat tissue with many passes, which may also improve tissue grafting and treatment longevity.[12] The main side-effect of the procedure is oedema, which is often dependent on injection volumes.[23] According to Coleman (2002), a minimum of 20 cc of centrifuged fat should be injected into each hand for significant improvement, but some patients may note that the resulting oedema lasts for up to 16 weeks.[2] In addition, this procedure is also very expensive.[10] In our experience, a standard treatment with CaHA requires two 1.5 mL vials and costs around €600 at the time of writing, although prices will vary from country to country. A survey among local plastic surgeons and dermatologists revealed that the cost of harvesting fat for autologous fat injection in Germany is, on average, over three-times the cost of one CaHA injection, although each injection using the harvested fat costs around half as much as one CaHA injection. Therefore, it would take several autologous fat injections to reach the break-even point, and the initial outlay is considerably higher compared with CaHA injections.
COLLAGEN
Collagen has been widely used as a dermal filler in cosmetic surgery, although it is not currently marketed. Bovine collagen has not been successful in correcting hand appearance due to its consistency, flow characteristics, lack of longevity and the resulting uneven skin surface.[7] However, recently, promising results with porcine collagen were reported.[11] For hand rejuvenation, the duration of effect of porcine collagen injection is yet to be reported. In the treatment of deep nasolabial wrinkles, porcine collagen lasted for up to 12 months; however, it should be noted that such results cannot be extrapolated to hand augmentation as the duration of effect in hands, which lack expression muscles, is likely to be different.[12]
HYALURONIC ACID
The ageing process results in the depletion of endogenous hyaluronic acid (HA), which has an important role in the dermal extracellular matrix for hydration, biomechanical integrity and oxidative stress protection.[1314] Addition of exogenous HA in vitro increases the proliferation of human fibroblasts[1516] and promotes endogenous HA production.[17] Thus, intradermal injection of native HA increases dermal thickness and elasticity.[1819] Hyaluronidase can also be used to reverse any unwanted effects of native HA dermal filler if needed.[20] Cross-linked HA, which is not degraded as quickly as native HA, has been shown to enhance the production of collagen in vivo[21] and can be injected as a volume filler subcutaneously. However, when using biphasic HA fillers [Table 2], injection in the deep dermis is necessary to avoid bluish skin discolouration due to the Tyndall effect. Adverse events can include the development of papules.[7] Additionally, research in facial HA fillers has shown adverse events related to excessive HA overcorrection,[22] and repeat injections may be needed in the event of undercorrection.[23] The duration of effect was not reported for hand volume restoration, but, for other indications, the effect lasted 6–12 months.[24–27]
CALCIUM HYDROXLYAPATITE
CaHA, an inorganic component in bone and teeth, can also be used as an inert and biocompatible dermal filler.[28] CaHA (Radiesse®, Merz Pharmaceuticals GmbH) is a high-viscosity, high-elasticity filler[29] that is generally injected alone, but premixing with the local anaesthetic lidocaine[1030] [Figure 1] was recently approved in the USA. CaHA can be titrated by mixing with lidocaine for optimal use in different areas.[29] The opacity and colour of CaHA blends well with the skin and conceals veins and tendons.[7] In addition, real-time correction is achieved[7] as no under- or overcorrection is required with CaHA.[31] The duration of hand volume restoration was reported to be more than 6 months[7283233] and, in other indications, up to 18 months.[34] Its long-lasting results may be due to neocollagenesis, which in laboratory studies continued for up to 72 weeks.[7] Treatment with CaHA results in little downtime for patients,[30] with only the usual adverse events described for dermal fillers, including bruising, oedema and tenderness.[72835] In one study,[10] three reported cases of delayed oedema were all self-resolved. In a study of 101 patients, high satisfaction with CaHA treatment was reported by both physicians and patients.[32]
![Procedure for mixing calcium hydroxylapatite (CaHA) with lidocaine:[30] (a) pull lidocaine into a 3-mL syringe, (b) connect the syringe to a connector, fill with lidocaine, (c) connect syringe containing CaHA to connector, (d) push contents of CaHA syringe into the syringe containing lidocaine, push plungers back and forth 310 times, inject with CaHA syringe](/content/173/2012/5/3/img/JCAS-5-163-g003.png)
- Procedure for mixing calcium hydroxylapatite (CaHA) with lidocaine:[30] (a) pull lidocaine into a 3-mL syringe, (b) connect the syringe to a connector, fill with lidocaine, (c) connect syringe containing CaHA to connector, (d) push contents of CaHA syringe into the syringe containing lidocaine, push plungers back and forth 310 times, inject with CaHA syringe
POLY-L-LACTIC ACID
Poly-L-lactic acid (PLLA) is a synthetic product that has been used for 30 years in surgical implants, and it has been hypothesized to stimulate collagen production.[936] Its use in hand rejuvenation has been previously reported.[93637] However, treatment requires multiple injections[7] and can therefore be expensive for patients.[10] Unlike other long-lasting fillers, treatment with PLLA entails a waiting period to ascertain full correction,[137] but no overcorrection is required.[8] The effect of PLLA has been shown to last for 18–24 months in indications other than hand volumization.[38] In addition to bruising and oedema, adverse events include the development of visible subcutaneous papules and the risk of persistent granuloma.[93639] These adverse events can be minimized by using a more diluted preparation with 7 mL of diluent per PLLA bottle[13] and ensuring massage during treatment followed by daily hand massage for 1 month posttreatment.[9]
INJECTION TECHNIQUES FOR HAND REJUVENATION
Knowledge of hand anatomy can influence the development of injection techniques. A recent report identified three distinct fatty laminae (superficial, intermediate and deep) divided by thin fascia on the dorsum of the hand.[40] The thickness of the superficial lamina seems to correlate with body mass index, and there are no vascular or neuronal structures in this lamina. The large dorsal veins and sensory nerves are located within the intermediate lamina, while the tendons are located in the deep lamina.[40] Theoretically, injection of dermal filler into the superficial lamina, above the veins, would best conceal the veins. However, to date, this has proved to be technically impossible without puncturing the veins. Injecting into the deep lamina towards the veins, above the metacarpal plane, is effective at concealing the veins, probably due to compression by the injected material [Figures 2 and 3]. Generally, dermal fillers are injected subdermally using a 25- to 32-gauge needle or a blunt cannula. The use of blunt cannulae, instead of sharp needles, minimizes the risk of damage to nerves and blood vessels.[2]
![Examples of dermal filler injection techniques for hand volume restoration: (a) tenting of the skin,[7] (b) microdroplet technique showing injection points at the dorsal hand (20 microdroplet injections per hand, random injection point distribution avoiding blood vessels),[41] (c) injection site forming a bolus of calcium hydroxylapatite mixture (0.5 mL bolus) in the areolar plane[7]](/content/173/2012/5/3/img/JCAS-5-163-g004.png)
- Examples of dermal filler injection techniques for hand volume restoration: (a) tenting of the skin,[7] (b) microdroplet technique showing injection points at the dorsal hand (20 microdroplet injections per hand, random injection point distribution avoiding blood vessels),[41] (c) injection site forming a bolus of calcium hydroxylapatite mixture (0.5 mL bolus) in the areolar plane[7]

- Bolus injection with calcium hydroxylapatite and lidocaine: A 54-year-old, treatment-naïve, female patient (a) before treatment, (b) after injection, in the central part of the dorsum of the hand and (c) after sitting on the hand for 10 min
The injection techniques reported for hand volume restoration include:
-
Tenting: injecting a single bolus by pinching the skin [Figure 2a].
-
Serial puncture: injecting the filler in a series of small volumes along a line.
-
Microdroplets: injecting minute amounts of filler at a large number of points [Figure 2b].[41]
-
Tunneling or linear retrograde threading: once the needle is at the appropriate depth, injecting the filler along a line in a retrograde fashion (i.e., while withdrawing the needle).
-
Fanning: without withdrawing the needle, several threads are injected radially.
For the single-bolus technique [Figure 2c], some physicians use premixed syringes with dermal filler and anaesthetic agent: CaHA[7102830] and PLLA.[9] Another technique consists of creating a bulla with a bolus of lidocaine and injecting the CaHA filler into the bulla; this is a quick, easy-to-administer technique that provides consistent results and positive patient feedback.[35] All fillers can cause swelling of the dorsum of the hands for several days. Bruising may also occur, but is rare with the single-bolus technique described in detail below. Massage can cause discomfort when performed too vigorously.
COMPARISON OF THE DIFFERENT METHODS
The dermal fillers and preferred injection techniques for hand volume restoration are summarized in Table 2.
PRACTICAL CONSIDERATIONS
Our focus as dermatologists is using minimally invasive techniques for hand augmentation. To date, we have treated around 50 cases of hand augmentation. At the present time, CaHA is our preferred filler for hand rejuvenation due to its high lifting capacity, viscosity and elasticity, and longevity due to stimulation of collagen production. We also use cross-linked HA as a filler for hand augmentation, while for treating dermal elastosis we use non cross-linked, native HA and an intradermal injection technique. This leads to smoothing and thickening of the skin without affecting the subdermal volume.[1819]
When using CaHA, diluting it with a local anaesthetic makes the procedure more comfortable for the patient. It also has the advantage of reducing the high viscosity of CaHA,[29] which allows for a more even distribution of the product. This is important because a homogenous distribution of the filler is more desirable when treating a large surface area with a rather thin subcutaneous layer of tissue such as the back of the hands compared with areas of the face, which are typically treated with dermal fillers. Standard practice is to add one part lidocaine to four parts CaHA; but in limited cases only, it might be useful to add more lidocaine to reduce viscosity further and thus facilitate a more even distribution of the product. Edelson[7] used 0.5 mL of lidocaine for 1.3 mL of CaHA, resulting in the addition of 38.4% of liquid volume. The process of diluting CaHA with the local anaesthetic is shown in Figure 1. Busso and Voigts[42] have shown that with 10 mixing passes, an even distribution of lidocaine in CaHA is achieved with the expected reduction in viscosity and extrusion force, but with no difference in needle jam rates, elasticity and pH compared with CaHA alone.
For hand augmentation, we generally use a 28-gauge, three-quarter-inch, thin-wall needle. The administration of a single bolus instead of several boluses, fanning, serial puncture or microdroplets reduces the risk of bruising as the number of injection sites is minimized. After the implantation of the bolus, the patients are advised to sit on the dorsum of their hands for 10 min. The pressure and warmth generated by this procedure flattens out the boluses considerably [Figure 3]. Subsequently, a massage of the dorsum of the hands is performed in the surgery until even distribution and filling is achieved. Examples of the results from this technique are shown in Figures 3–5. Figures 4b and 4c show a clear improvement after 6 weeks and 6 months compared with before treatment [Figure 4a]; the tendons are less visible and fine wrinkles have been ameliorated, representing dermal elastosis. Figure 5b shows a similar improvement over baseline [Figure 5a] in another patient 6 months after treatment. Our current practice is to administer up to 0.8 mL of local anaesthetic, which enables an even easier spread of the product after sitting on the hand and massaging. The beneficial results of this technique typically last for at least 1 year.

- Injection with calcium hydroxylapatite (1.5 mL) and prilocaine (0.3 mL) in each hand: A 62-year-old female patient (a) before treatment, (b) 6 weeks after treatment and (c) 6 months after treatment
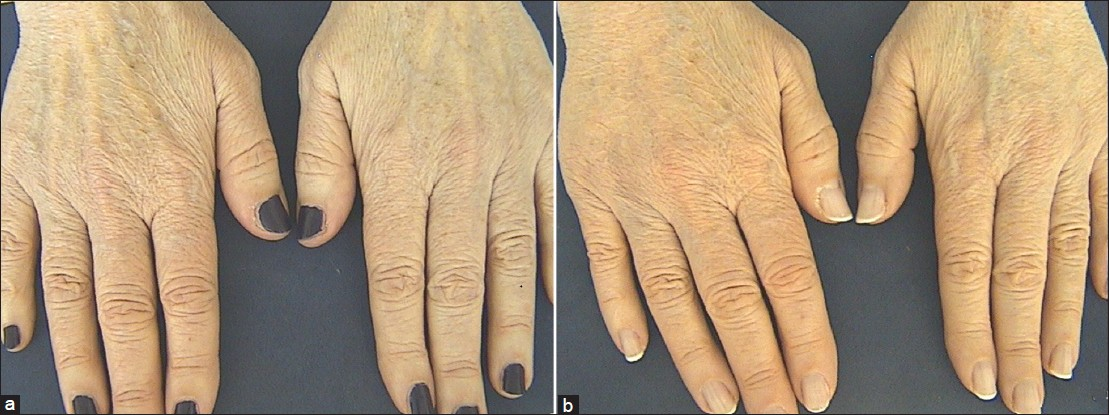
- Injection with calcium hydroxylapatite (1.5 mL) and prilocaine (0.3 mL) in each hand: A 65-year-old female patient (a) before treatment and (b) 6 months after treatment
SUMMARY
A number of long-lasting dermal fillers have been used for hand rejuvenation. Their characteristics and corresponding injection techniques allow the physician to tailor the treatment to the individual's needs.
ACKNOWLEDGEMENTS
Editorial assistance was provided by Ogilvy 4D, Oxford, UK, supported by Merz Pharmaceuticals GmbH.
Source of Support: Ogilvy 4D, Oxford, UK, supported by Merz Pharmaceuticals GmbH.
Conflict of Interest: Both authors have acted as consultants, given expert testimony and received honoraria for Merz Pharmaceuticals GmBH, Frankfurt, Germany, Procutis GmbH, Bad Soden, Germany in the last 3 years.
REFERENCES
- Hand rejuvenation with structural fat grafting. Plast Reconstr Surg. 2002;110:1731-44.
- [Google Scholar]
- Structural and functional changes of normal aging skin. J Am Acad Dermatol. 1986;15:571-85.
- [Google Scholar]
- Hand recontouring with calcium hydroxylapatite (Radiesse®) J Cosmet Dermatol. 2009;8:44-51.
- [Google Scholar]
- An Overview of Permanent and Semipermanent Fillers. Plast Reconstr Surg. 2006;118:7S-14S.
- [Google Scholar]
- Addressing volume loss in hand rejuvenation: A report of clinical experience. J Cosmet Laser Ther. 2008;10:237-41.
- [Google Scholar]
- Multinational, multipatient study of calcium hydroxylapatite for treatment of the aging hand: European Cosmetic Physician Group on Hand Augmentation. Dermatol Surg. 2010;36:782-9.
- [Google Scholar]
- Nonsurgical hand rejuvenation with Dermicol-P35 30G. Aesthet Surg J. 2009;29:S19-S21.
- [Google Scholar]
- Twelve-month persistency of a novel ribose–cross-linked collagen dermal filler. Dermatol Surg. 2008;34:S31-S9.
- [Google Scholar]
- Hyaluronan-mediated protective effect against cell damage caused by enzymatically produced hydroxyl (OH·) radicals is dependent on hyaluronan molecular mass. Cell Biochem Funct. 1994;12:281-8.
- [Google Scholar]
- Hyaluronan: from extracellular glue to pericellular cue. Nature Reviews Cancer. 2004;4:528-39.
- [Google Scholar]
- Behaviour of fibroblasts and epidermal cells cultivated on analogues of extracellular matrix. Biomaterials. 1988;9:91-6.
- [Google Scholar]
- Hyaluronan used for intradermal injections is incorporated into the pericellular matrix and promotes proliferation in human skin fibroblasts in vitro. Dermatology. 2010;221:219-28.
- [Google Scholar]
- The synthesis of hyaluronic acid by human synovial fibroblasts is influenced by the nature of the hyaluronate in the extracellular environment. Rheumatol Int. 1987;7:113-22.
- [Google Scholar]
- Einsatz biophysikalischer Messverfahren zur Untersuchung der hautphysiologischen Wirkung injizierbarer Hyaluronsäure. Der Hautarzt. 2007;58:1046-50.
- [Google Scholar]
- Recovery of skin elasticity and turgor by intradermal injection of hyaluronic acid (Ial-System®) by the cross-linked technique. G Ital Dermatol Venereol. 2001;136:187-94.
- [Google Scholar]
- The use of hyaluronidase to reverse the effects of hyaluronic acid filler. Plastic Reconstructive Surgery. 2004;114:277.
- [Google Scholar]
- In vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143:155-63.
- [Google Scholar]
- Hyaluronidase offers an efficacious treatment for inaesthetic hyaluronic acid overcorrection. J Cosmet Dermatol. 2007;6:159-62.
- [Google Scholar]
- Nonsurgical management of upper eyelid margin asymmetry using hyaluronic acid gel filler. Ophthal Plast Reconstr Surg. 2011;27:1-3.
- [Google Scholar]
- Persistence and improvement of nasolabial fold correction with nonanimal-stabilized hyaluronic acid 100,000 gel particles/mL filler on two retreatment schedules: results up to 18 months on two retreatment schedules. Dermatol Surg. 2008;34:S2-8.
- [Google Scholar]
- Effectiveness of Juvéderm Ultra Plus dermal filler in the treatment of severe nasolabial folds. Plast Reconstr Surg. 2008;121:289-97.
- [Google Scholar]
- Juvederm injectable gel: A multicenter, double-blind, randomized study of safety and effectiveness. Aesthet Surg J. 2008;28:17-23.
- [Google Scholar]
- Hyaluronsäurefiller zur Korrektur der Nasolabialfalten – Ergebnisse einer klinischen Studie. Journal der Deutschen Dermatologischen Gesellschaft. 2008;6:S10-S4.
- [Google Scholar]
- A five-patient satisfaction pilot study of calcium hydroxylapatite injection for treatment of aging hands. Dermatol Surg. 2009;35:1978-84.
- [Google Scholar]
- Comparison of the rheological properties of viscosity and elasticity in two categories of soft tissue fillers: calcium hydroxylapatite and hyaluronic acid. Dermatol Surg. 2010;36:1859-65.
- [Google Scholar]
- Hand augmentation with Radiesse® (Calcium hydroxylapatite) Dermatologic Therapy. 2007;20:385-7.
- [Google Scholar]
- Calcium hydroxylapatite for facial rejuvenation. Semin Cutan Med Surg. 2006;25:132-7.
- [Google Scholar]
- Multicenter, randomized trial assessing the effectiveness and safety of calcium hydroxylapatite for hand rejuvenation. Dermatol Surg. 2010;36:790-7.
- [Google Scholar]
- A 52-week study of safety and efficacy of calcium hydroxylapatite for rejuvenation of the aging hand. J Drugs Dermatol. 2011;10:47-51.
- [Google Scholar]
- Long-lasting results with hydroxylapatite (Radiesse®) facial filler. Plast Reconstr Surg. 2006;118:15S-21S.
- [Google Scholar]
- A novel approach to treatment of the aging hand with Radiesse. J Drugs Dermatol. 2009;8:1122-6.
- [Google Scholar]
- Soft-tissue augmentation and the role of poly-L-lactic acid. Plast Reconstr Surg. 2006;118:46S-54S.
- [Google Scholar]
- Cosmetic use of polylactic acid for hand rejuvenation: report on 27 patients. J Cosmet Dermatol. 2006;5:233-8.
- [Google Scholar]
- ASDS guidelines of care: Injectable fillers. Dermatol Surg. 2008;34(Suppl 1):S115-48.
- [Google Scholar]
- Dorsal hand anatomy relevant to volumetric rejuvenation. Plast Reconstr Surg. 2010;126:163-8.
- [Google Scholar]
- Changes in skin physiology and clinical appearance after microdroplet placement of hyaluronic acid in aging hands. J Cosmet Dermatol. 2009;8:216-25.
- [Google Scholar]
- An investigation of changes in physical properties of injectable calcium hydroxylapatite in a carrier gel when mixed with lidocaine and with lidocaine/epinephrine. Dermatol Surg. 2008;34:S16-S24.
- [Google Scholar]




