
Translate this page into:
Dumbbell-Shaped Neurofibroma Over the External Ear
Address for correspondence: Dr. Srinivas Kodaganur, Junior Resident, #41, Vivek Boys’ Hostel, Karnataka Institute of Medical Sciences (KIMS) Campus, Vidyanagar, Hubli - 580 022, Karnataka, India. E-mail: srinirocks89@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Dumbbell-shaped swellings in neurofibroma have been commonly described in the spine, thorax, cranial cavity, and pelvis; however, dumbbell-shaped swellings in the peripheries are rare. Here, we report a dumbbell-shaped neurofibroma over the pinna in an 18-year-old female patient, its successful surgical management, and its association with Hashimoto thyroiditis.
To the best of our knowledge, this is the first ever case to be reported of a dumbbell-shaped neurofibroma over the external ear and only the fourth case of neurofibromatosis type 1 (NF1) to be associated with Hashimoto thyroiditis.
Keywords
Dumbbell-shaped neurofibroma
external ear
neurofibromatosis (NF)
neurofibromatosis 1 (NF1)

INTRODUCTION
Neurofibromatosis (NF) is one of the most common genetic disorders transmitted in an autosomal dominant fashion affecting more than 1 out of 3,000[1] individuals caused due to deletions, insertions, or mutations in neurofibromatosis type 1 (NF1) gene located in the pericentromeric region on chromosome 17.[2] It is characterized by the presence of cafe au lait spots, axillary freckling, neurofibromas, Lisch nodules, optic nerve gliomas, skeletal abnormalities, and malignant peripheral nerve sheath tumors.[3] Neurofibromas usually occur over the extremities and the trunk and also over the external auditory canal and can cause unilateral conductive hearing loss[4] but are rarely reported in the literature.
Here we describe an unusual presentation of dumbbell-shaped neurofibroma over the pinna, completely obstructing the external auditory canal with the extension to the retroauricular region.
CASE REPORT
A female patient aged 18 years presented with a swelling over the left ear of 1-year duration associated with decreased hearing. Clinical examination revealed a soft swelling measuring about 2 cm × 2 cm obliterating the concha of the left ear and the external auditory canal [Figure 2a]. Similarly, there was another soft swelling of 3 cm × 2 cm in the retroauricular region completely obliterating the retroauricular groove [Figure 2b]. There were multiple cafe au lait macules of varying sizes over the body. There was also a diffuse thyroid swelling involving both the lobes with no apparent nodularity. On subjecting the patient to slit-lamp examination, there were multiple Lisch nodules over both the irises. Tuning fork tests revealed mild conductive hearing loss in the left ear. Fine-needle aspiration cytology (FNAC) of the thyroid swelling showed features suggestive of Hashimoto thyroiditis [Figure 4b].

- Clinical photograph of the patient with her mother
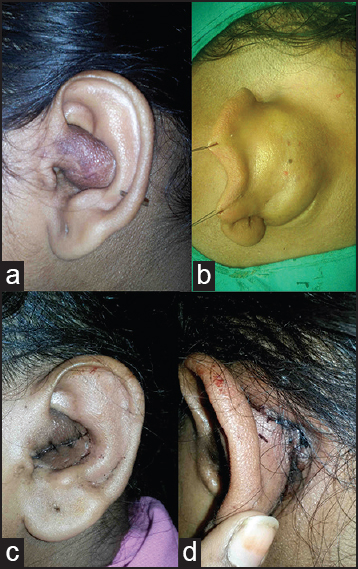
- (a) Preoperative clinical photograph of the pinna (anterior) (b) Preoperative clinical photograph of the pinna (posterior) (c) Postoperative clinical photograph of the pinna (anterior) (d) Postoperative clinical photograph of the pinna (posterior)
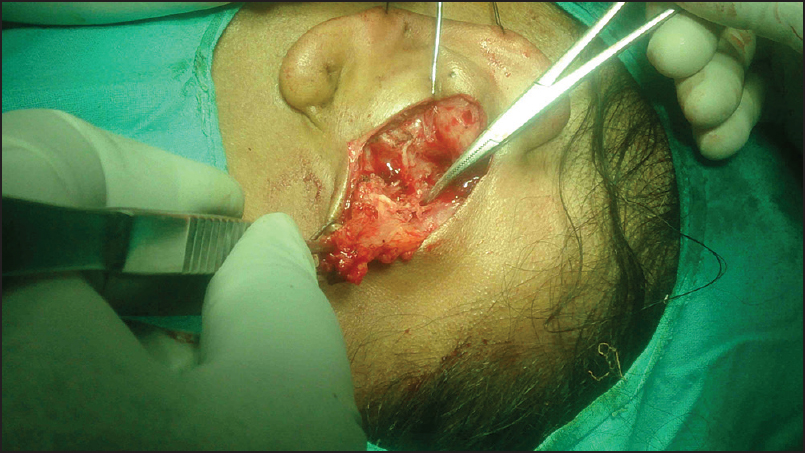
- Intraoperative photograph showing the tumor being excised and the forceps pointing toward the transcartilaginous extension
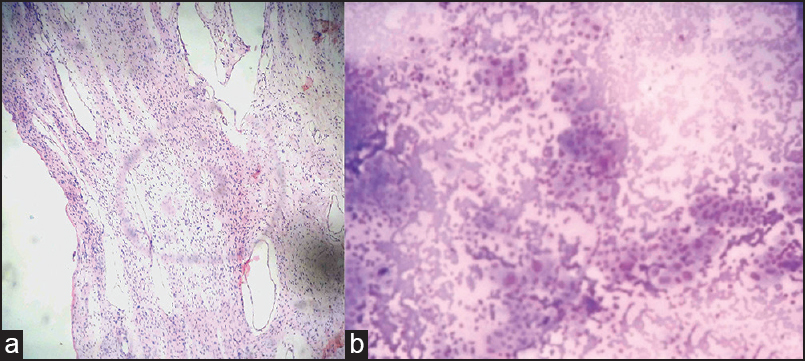
- (a) Histopathology of neurofibroma (b) Histopathology of Hashimoto thyroiditis
The mother of the patient had a large swelling over the right upper eyelid that completely obscured her vision [Figure 1].
Magnetic resonance imaging (MRI) showed a soft tissue swelling in the left external ear with diffuse enhancement and no intracranial extension [Figure 5b]. There was also an ill-defined lesion in the posterior part of the left thalamus with mild mass effect, suggestive of astrocytoma [Figure 5a].
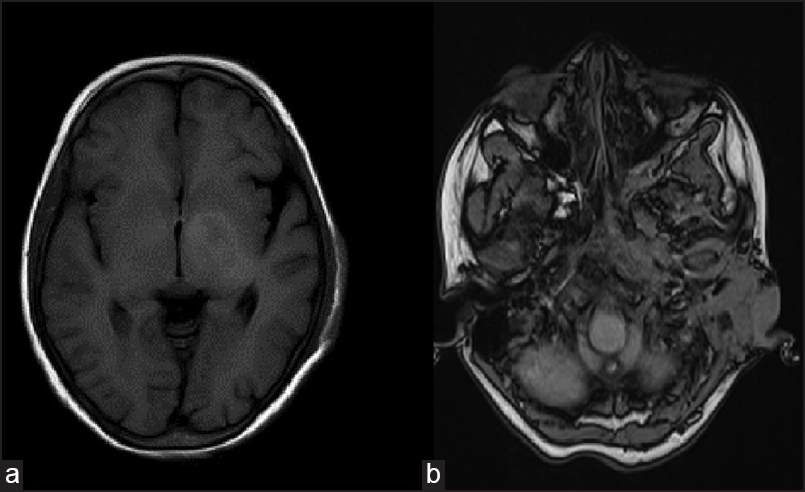
- MRI images showing (a) swelling over the external ear (b) ill-defined lesion in the thalamic region suggestive of astrocytoma
The patient was operated under general anesthesia. A curvilinear incision of 3 cm was taken over the swelling in the retroauricular region. The swelling was identified and dissected from the surrounding tissue. There was no identifiable capsule and on further dissection, there was a transcartilaginous extension of the swelling into the external auditory canal [Figure 3]. Posterior component of the swelling was excised. Swelling over the cymba was approached through an anterior incision.
The sutures were removed on postoperative day 5 and the result was cosmetically acceptable [Figure 2c and d].
Histopathological examination of the tissue showed numerous loosely spaced, wavy, spindle-shaped cells with pointed ends over a fibrillar background without a capsule, among which were interspersed numerous endothelial-lined spaces suggestive of neurofibroma [Figure 4a].
Informed consent was taken from the subjects according to the guidelines given in the Helsinki Declaration.
DISCUSSION
Dumbbell-shaped tumors have been commonly described in the spine, thorax, intracranial region, pelvis, and hand.[56789] However, dumbbell-shaped tumors in the periphery are rarely described in the literature.
Histologically, dumbbell-shaped tumors can be neurofibromas, neurilemmomas, lipomas, or paragangliomas.[56789] Dumbbell-shaped neurilemmomas have been described in the hand and are characterized by mild, localized pain, and paresthesia resulting from pressure on the nerve of origin and histologically they are well-encapsulated in contrast to neurofibromas that are usually painless and do not have a well-defined capsule.
Neurofibromas can occur in the thyroid gland, causing thyroid enlargement[10] but an association of Hashimoto thyroiditis with NF is extremely rare and has been described in only three cases in the literature.[11]
Indications for surgical removal of neurofibromas include cosmetic disfigurement or compression effects.
The indication in this case was both for cosmetic disfigurement and improvement in hearing.
Posterior and anterior approaches were used in this case since on posterior dissection, the swelling was found to be eroding the cartilage and extending anteriorly through a small communication. The anteriorly placed part of the swelling could not be extracted without creating a large defect in the cartilage. Hence, a small anterior incision was used.
After a thorough search of the literature using PubMed, Science Direct, and Google Scholar [Last accssed on 2015 30 Apr], we came to a conclusion that this is the first case to be reported of a dumbbell-shaped neurofibroma over the pinna.
This patient's mother who also had a plexiform neurofibroma over the right eyelid did not give consent for surgery.
Genetic counseling forms an important part of NF management since it is an autosomal dominant disease with 100% penetrance with variable expression.[3]
The affected individual can manifest merely with insignificant cafe au lait macules to large neurofibromas in the spinal canal with grave prognosis. These patients need to be counseled regarding the different manifestations of the disease so that an early intervention can prevent further complications.
CONCLUSION
Dumbbell-shaped neurofibromas over the ear have never been reported in the English literature to the best of our knowledge. This is the first case to be reported with successful excision providing an acceptable cosmetic and functional outcome and only the fourth case in the literature to be reported to have an association with Hashimoto thyroiditis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We would like to thank Dr. Ishwar R. Hosamani, Professor of the Department of General Surgery, Dr. Choukimat S, Professor of the Department of Pathology, and Dr. Anirudha Kulkarni, Associate Professor of the Department of Neurosurgery, Karnataka Institute of Medical Sciences, Hubli for their help in successful completion of the manuscript.
References
- A genetic study of von Recklinghausen neurofibromatosis in south east Wales. I. Prevalence, fitness, mutation rate, and effect of parental transmission on severity. J Med Genet. 1989;26:704-11.
- [Google Scholar]
- Deletions and a translocation interrupt a cloned gene at the neurofibromatosis type 1 locus. Cell. 1990;62:187-92.
- [Google Scholar]
- A clinical study of type 1 neurofibromatosis in north west England. J Med Genet. 1999;36:197-203.
- [Google Scholar]
- Plexiform neurofibroma in the ear canal of a patient with type I neurofibromatosis. Braz J Otorhinolaryngol. 2009;75:158.
- [Google Scholar]
- Dumbbell-shaped neurofibroma of the upper thoracic spine: A case report. South Asian J Cancer. 2013;2:226.
- [Google Scholar]
- Solitary benign schwannomas in major nerve systems of the head and neck. J Craniofac Surg. 2009;20:957-61.
- [Google Scholar]
- Asynchronous abdomino-parasacral resection of a giant pelvic lipoma protruding to the left buttock. Int J Surg Case Rep. 2014;5:975-8.
- [Google Scholar]
- Posterior mediastinal paragangliomas: A report of three patients with peculiar tumours. Respirology. 2009;14:459-61.
- [Google Scholar]
- Neurofibromatosis type 1 associated with Hashimoto's thyroiditis: Coincidence or possible link. Case Rep Neurol Med 2013 2013:910656.
- [Google Scholar]




