
Translate this page into:
Granular Cell Tumour
Address for correspondence: Dr. Hemant Kumar Singh, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry - 605 006, India. E-mail: hemant7771@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Dear Editor,
Granular cell tumour is a benign tumour of Schwann cell origin. It can occur in skin, subcutaneous tissue, submucosa, and deep soft tissue and internal organs but is most common in head and neck region particularly tongue. Rarely, has it been documented to present as an inguinal swelling.[1234]
A 13-year-old boy presented with a gradually increasing swelling in the left inguinal region for two years. This was associated with a dull aching pain. He had no significant illnesses in the past or any familial diseases.
His general examination was unremarkable. Local examination revealed a swelling of 3 × 2 cm in the left inguinal region near the root of penis [Figure 1a]. It was non-tender, firm and mobile. There was no impulse on cough. The cord structures, testes and external genitalia were normal. Ultrasonography of the abdomen was normal. Ultrasound of the swelling showed a hypoechoic lesion of 1.2 cm with loss of fatty hilum. Both the testes and epididymis were normal. A provisional diagnosis of an enlarged inguinal lymph node was made. Fine needle aspiration cytology showed uniform appearing large polyhedral cells arranged in sheets. These cells had small round nuclei and abundant dense granular cytoplasm. These features suggested a possibility of a granular cell tumour.
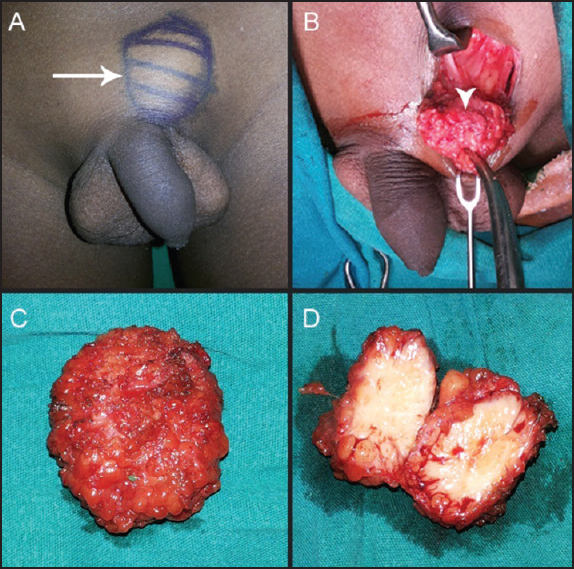
- (a) Clinical photograph showing a swelling in the left inguinal region near the root of the penis (b) Intraoperative appearance of the tumour (c) Tumour after en bloc excision (d) Cut section of the tumour showing solid areas with interspersed fatty tissue
Since the patient was symptomatic, a decision to excise the swelling was made. Intra-operatively, the swelling (3 × 3cm) was in the subcutaneous plane in the inguinal region [Figure 1b]. It was adherent to the external oblique aponeurosis. Enbloc excision of the swelling was done. On cut section, the tumour showed solid areas with interspersed fatty tissue [Figure 1c and d]. Histopathology confirmed the findings of cytology. All margins were free of the tumour. Immunohistochemistry was positive for S100 protein [Figure 2]. Post-operatively, the wound healed well with no complications. The patient was advised a regular yearly follow-up.
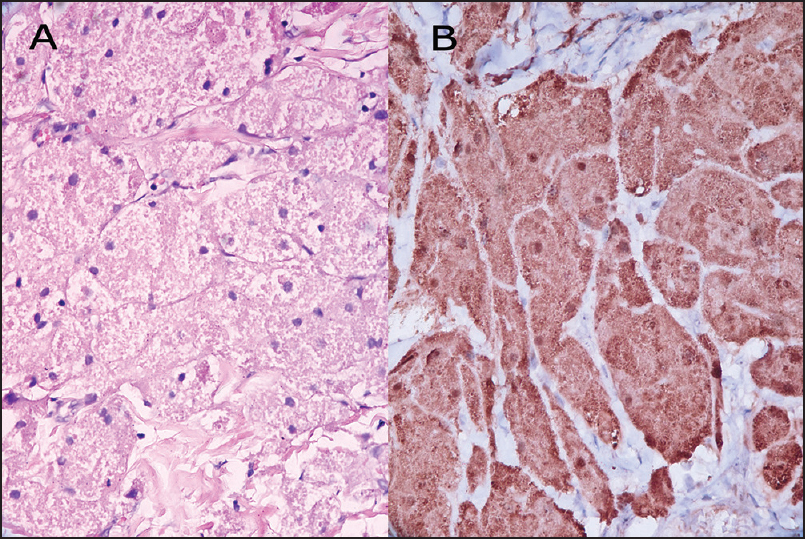
- (a) (400X) Haematoxylin and Eosin staining of the tumour showing large polyhedral cells arranged in sheets with abundant granular cytoplasm and small hyperchromatic nuclei (b) (400X) Immunohistochemistry showing positivity for S100 protein suggestive of a granular cell tumour
The common causes of inguinal swelling in adolescents include lipoma, fibroma, fibrolipoma, dermatofibroma, hamartoma, lymphatic or venous malformations. Rarely, as seen in present case, granular cell tumour has been documented to present as inguinal swelling. It commonly affects third to fourth decades of life. However, the present patient was much younger. Familial associations are infrequent. These neoplasms are usually small ranging in size from 5 mm to 2 cm and slow growing. They are well-circumcised and firm.
These tumours are non-encapsulated and composed of irregularly arranged sheets of large polyhedral cells with small central hyperchromatic nuclei and abundant eosinophilic, PAS-positive granular cytoplasm. The overlying epithelium often shows prominent pseudo-epitheliomatous hyperplasia, which may be misdiagnosed as squamous cell carcinoma if a superficial biopsy is taken for examination. Recent studies on ultrastructure and immunohistochemistry have proven it to be of Schwann cell differentiation. The cells are positive for S-100, CD68, protein gene product 9.5, and inhibin-alpha.[5]
The malignant counterparts of these tumours are exceedingly rare. The treatment of choice for benign tumours is observation or wide local excision. Recurrent granular cell tumours may benefit from adjuvant radiotherapy.[6] Chemotherapy has shown promise in metastatic granular cell tumour.[7] In this patient, the tumour was excised enbloc and histopathology was suggestive of a benign tumour with tumour-free margins. So, the patient was asked to follow-up annually.
Granular cell tumour being rare in the inguinal region, is usually not suspected clinically and the diagnosis is usually made on histopathology/cytology.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Granular cell tumour of the soft tissues: A case report and literature review. Int Semin Surg Oncol. 2006;3:21.
- [Google Scholar]
- Granular cell tumor — clinically presented as lymphadenopathy. Coll Antropol. 2010;34:261-3.
- [Google Scholar]
- Granular cell tumor in inguinal region: A case of mistaken identity on cytology. J Cytol. 2012;29:60-2.
- [Google Scholar]
- Histologic and immunohistochemical profiles of benign granular cell tumors. Report of 41 cases. Ann Pathol. 1995;15:198-202.
- [Google Scholar]
- Gemcitabine plus paclitaxel may be a promising chemotherapy regimen for metastatic granular cell tumour. Clin Oncol (R Coll Radiol). 2008;20:93-6.
- [Google Scholar]




