
Translate this page into:
“Jigsaw Puzzle” Advancement Flap for the Reconstruction of an Infraorbitary Defect
Address for correspondence: Dr. Diogo Cerejeira, Dermatology Department of Hospital Garcia de Orta, Avenida Torrado da Silva, 2805-267 Almada, Portugal. E-mail: diogo_cerejeira@hotmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Sir,
Defects involving the infraorbitary region are relatively common in dermatological surgery, especially after tumor ablation. Improper reconstruction of these defects may lead to the retraction of the lower eyelid and eventual ectropion. Many variations of “jigsaw puzzle” advancement flap have already been described to cover different facial defects. However, to the best of authors’ knowledge, there is no report related to its usage in the infraorbitary region.
A 72-year-old woman was referred to our Dermatologic Surgery Department due to a squamous cell carcinoma in the left infraorbitary region, confirmed by skin biopsy. The tumor and a margin of 5 mm were excised under local anesthesia (2% lidocaine with epinephrine 1:100,000) resulting in a 1.7 × 1.4 × 0.9 cm defect. Using a template of the defect, we designed an inferior-based advancement flap with the dog-ears laterally along the relaxed skin tension lines (RSTL) [Figure 1A]. The dog-ears were excised, and the underlying fat was trimmed off the flap [Figure 1B]. The secondary defects were closed with 4/0 subcutaneous sutures from advancing the cheek skin to the periosteum of the maxillary bone. The flap was then pulled upwards into position on the infraorbitary defect. Finally, all the wounds were closed using a 5/0 non-absorbable, sterile monofilament suture [Figure 1C]. No post-operative complications were noted. One week after surgery, an excellent cosmetic outcome was observed [Figure 1D].
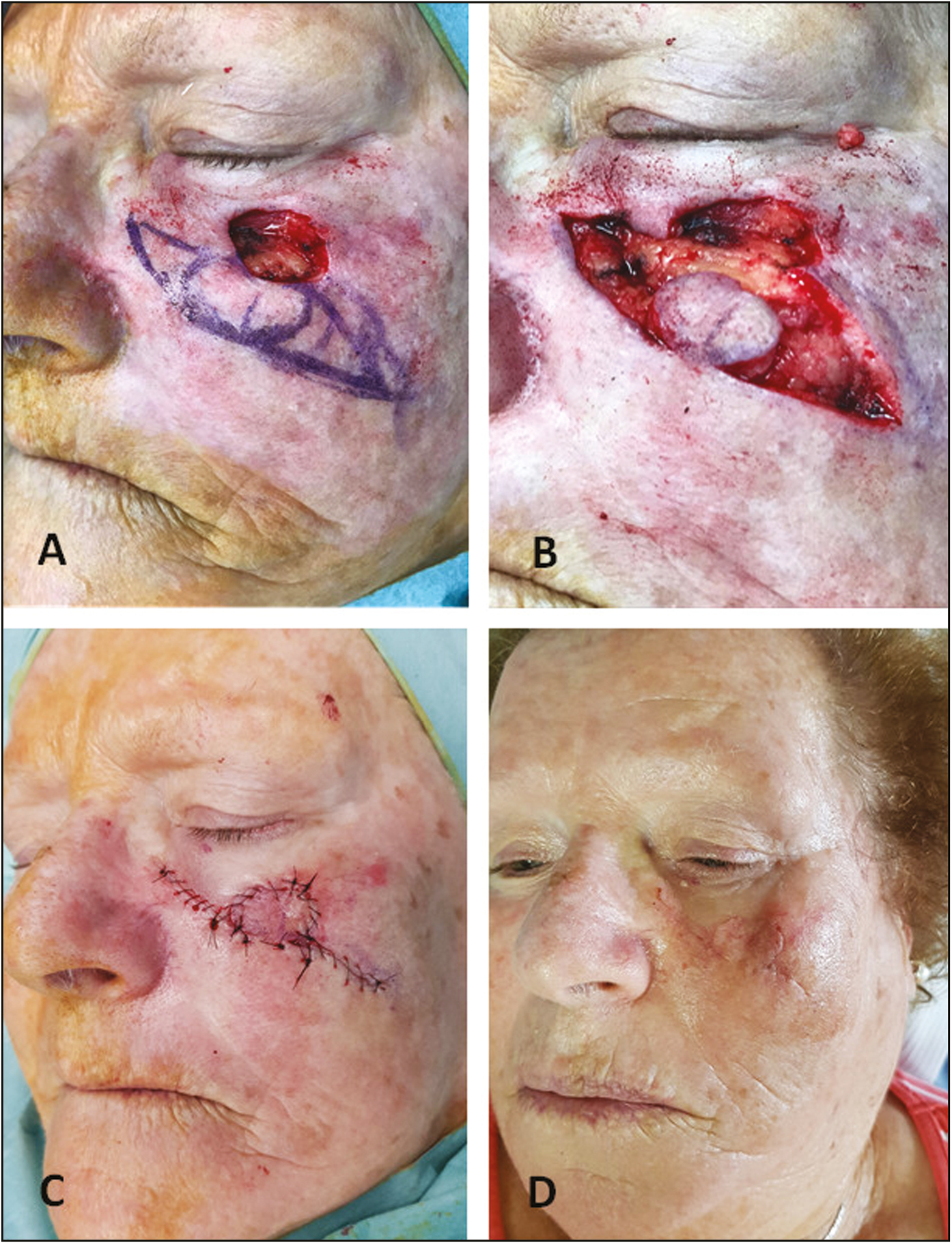
- (A) Clinical picture of the infraorbitary defect and the surgical planning with “jigsaw puzzle” advancement flap. (B) Secondary defect after the excision of ear-dogs. (C) Final intraoperative result. (D) One-week follow-up
The reconstruction of the infraorbitary region should combine restoration of adequate function and a satisfactory aesthetic outcome. Although several repair options are available, the formation of post-operative ectropion due to scar contracture is not uncommon.
Originally described by Goldberg et al.[1] in 2005, the “jigsaw puzzle” advancement flap has been successfully used to repair different sorts of defects located in the nose, upper lip, and retroauricular region.[123] However, the execution of this flap for the reconstruction of infraorbitary defects also offers numerous advantages, in comparison to possible alternative techniques. When correctly performed, this procedure allows the mobilization of a broad donor area (redundant skin of the cheek) into a round or rectangular defect, with minimal distortion or tension. The appropriate blood supply and lymphatic drainage are guaranteed by a large pedicle flap, which reduces eventual flap distress. Moreover, the dog-ears can be placed along with the RSTL, leading to a proper healing process and excellent aesthetic results. A key point in the execution of this flap is the anchoring of the subcutaneous sutures to the maxillary periosteum. This avoids the creation of vertical stress vectors that would possibly contribute to the formation of post-operative ectropion. To minimize the risk of causing a “trapdoor” deformity, the dimension of the flap should not be larger than the defect and its subcutaneous fat should be meticulously trimmed.
We highlight in our case a new application of “jigsaw puzzle” advancement flap to repair small-to-medium defects of the infraorbitary region with optimal aesthetic and functional results.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- “Jigsaw puzzle” advancement flap for repair of a surgical defect involving the lateral nasal ala. Dermatol Surg. 2005;31:569-71.
- [Google Scholar]
- The “jigsaw puzzle” advancement flap for reconstruction of a retroauricular surgical defect. J Drugs Dermatol. 2013;12:115-6.
- [Google Scholar]




