
Translate this page into:
Penis Girth Augmentation Using SEPA Flap and Dermofat Grafts
Address for correspondence: Dr. Souvik Adhikari, 154A Diamond Harbour Road, Kolkata 700060, India. E-mail: souvikadhikari@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
Men of various ages feel that an increase in penile size would give them and their sexual partners an increased confidence. There are a variety of methods for increasing penile girth, such as injection therapies and surgery. All of these methods have a high complication rate which must be emphasized to the patients. In this article, the techniques used for increasing penile girth using dermofat grafts and SEPA (superior external pudendal artery) flaps are highlighted along with their complications and their management thereof.
Patients and Methods:
Ten patients were operated for penile girth augmentation between June 2016 and March 2022. Of these, six patients had augmentation using dermofat grafts and four patients had SEPA flaps. Patients were chosen as per the Augmentation Phalloplasty Patient Selection and Satisfaction Inventory (APPSSI) score which was between 2 and 6 in the pre-operative period. The age range of the patients were between 25 and 57 years. The mid-penile girth in the flaccid state ranged from 8.8 to 12.3 cm.
Results:
Post-operatively, after 6 months, the final girth increase varied from 1.9 to 2.6 cm. The complication rate was 50% and included skin loss, urinary obstruction, fat necrosis, and so on. The post-operative APPSSI score ranged from 2 to 12. Complications were more in uncircumcised patients and in those who desired excessive augmentation.
Conclusion:
Penis girth augmentation using SEPA flaps and dermofat grafts is indicated in patients who fulfill the criteria and give appreciable girth increase, but patients need to be aware of the potential complications of these surgeries.
Keywords
Cosmetic penis surgery
dermofat
penis augmentation
penis girth
penis surgery
SEPA flap

BACKGROUND
There is a sense of insecurity among men of various ages regarding their penile size, which has increased owing to the effects of pornography. Patients are concerned regarding their penile length as well as girth and think that increasing these parameters would give them a sense of confidence and also to their sexual partners.[1] Most of these patients have normal-sized penis but they would still want an increase.[2] It may be mentioned here that there is no absolute fixed penis size in males and penile size measurement reveals a continuum. Whether or not a person has normal penile size is determined from charts which have a mean penile size and standard deviations based on population measurements.
There are a variety of procedures employed for increasing penile girth. The simplest is injection of silicone, hyaluronic acid, or fat into the penis.[3456] More invasive procedures incorporate a variety of substances into the penis including dermal strips, dermofat strips, allografts, and silicone penile implants inserted into the subcutaneous space.[7] Published literature has highlighted the high rate of complications associated with these surgical procedures.[7] These include but are not restricted to wound complications, post-operative curvature problems of the penis, impaired penile sensation, shortening of the penis, problems with erection, sexual dysfunction, and so on. It is therefore important that patients be appropriately educated regarding these potential complications that may arise as a result of this form of surgery and only proceed to surgery if they agree despite having an adequate knowledge of the same.
The purpose of this article is to highlight the techniques employed in increasing girth of the penis using SEPA (superior external pudendal artery) flaps and dermofat grafts, the subsequent complications thereof, and the management of the same.
PATIENTS AND METHODS
Between June 2016 and March 2022, 54 patients were screened using the Augmentation Phalloplasty Patient Selection and Satisfaction Inventory (APPSSI) and of these, 10 patients were selected and operated on by the author in his private surgical practice. Patients were taken up for surgery if they had a score between 0 and 6. In the rest, proper counseling was done and surgery refused. Of these, 6 patients had dermofat grafting to the penis and 4 patients had SEPA flap augmentation of the penis. All procedures performed in this study were in accordance with ethical standards of the Helsinki Declaration and its later amendments or comparable ethical standards.
The age of the patients varied from 25 to 57 years. The mid-penile circumference was measured in all patients in the flaccid state which ranged from 8.8 to 12.3 cm (mean 9.8 cm). Two patients who were operated on by the author previously for a penile length increase subsequently requested for a dermofat augmentation of penile girth and one patient opted for penile length as well as girth increase using SEPA flap in the same sitting [Table 1].
| Sr. no. | Age | Technique | Complications | Pre-op penile girth (cm) | Post-op penile girth (6 months) | Pre-op APPSSI score* | Post-op APPSSI score (6 months) |
|---|---|---|---|---|---|---|---|
| 1 | 26 | Dermofat | Partial foreskin loss | 9.1 | 11.7 | 2 | 12 |
| 2 | 25 | Dermofat | None | 11.3 | 13.4 | 4 | 10 |
| 3 | 32 | Dermofat | None | 10.2 | 12.1 | 4 | 9 |
| 4 | 28 | Dermofat | Fat necrosis with exudation | 8.8 | 11.2 | 5 | 9 |
| 5 | 24 | SEPA† | None | 9 | 11.2 | 3 | 12 |
| 6 | 57 | Dermofat | None | 9.8 | 10.8 | 5 | 11 |
| 7 | 32 | SEPA + ligament release | Skin loss with fat necrosis and exudation | 9.4 | 11.4 | 6 | 6 |
| 8 | 26 | SEPA | None | 12.3 | 14.2 | 6 | 11 |
| 9 | 34 | Dermofat | Fat necrosis with exudation | 9.6 | 11.9 | 4 | 8 |
| 10 | 25 | SEPA | Skin loss, urinary blockage from severe foreskin swelling, and urine track through wound | 8.9 | 11.2 | 3 | 2 |
*Augmentation Phalloplasty Patient Selection and Satisfaction Inventory
†Superior external pudendal artery flap
Patients were informed about the various processes of penile girth augmentation surgery and their merits and demerits and were especially counseled that their penile girth was within normal limits as per population study. The high likelihood of complications was informed to them as well as the orientation of scars. Informed consent was then obtained from the patients and the appropriate procedure conducted under local anesthesia without any form of sedation in all patients with top-up anesthesia whenever required. Injections were given in the deeper plane first and then into the superficial plane. The technique of performing this surgery exclusively under local anesthesia in an outpatient setting was influenced by the previous work of Hsu et al.[8]
The APPSSI score was again used to measure the outcome of surgery 6 months after the procedure. The APPSSI score of patients being considered for surgery ranged from 2 to 6. Follow-ups were performed at 3 and 6 months after the procedure apart from complication management as many patients were lost to follow-up after that period.
Technique of dermofat grafting
Patients were given the option of harvesting of dermofat grafts from various anatomical locations and all of them opted for the lower abdomen. All surgeries were performed under local anesthesia without any form of sedation. Three patients were circumcised and three patients were uncircumcised.
The mid-penile girth was measured in the flaccid state, and the width of the dermofat graft was determined by extrapolating the measured penile girth on to the lower abdomen excluding the width of the urethra as the dermofat graft would be sparing this area. The stretched penile length calculation (from the root of the penis to the coronal sulcus) was used to determine the length of the dermofat graft. Local anesthesia was then injected in the area of the proposed donor dermofat site in the form of lidocaine 2% with epinephrine 1:200,000 diluted 1:1 with normal saline.[910] Subsequently, undiluted lidocaine 2% was used for dorsal penile nerve block, injecting on either side of the suspensory ligament supplemented with a ring block. Around 5 mL of 2% lidocaine was used for the penile nerve blocks. A waiting time of 10 min was given.
The incisions were first made around the circumference of the proposed dermofat harvesting zone, and de-epithelialization was done taking care that hair follicles encountered were removed adequately [Figure 1]. Following this, the incisions were deepened into the superficial layer of subcutaneous fat and around 3–5 mm of fat was harvested along with the dermis. Scarpa’s fascia was not violated. The adjacent areas were then mobilized adequately and the wound was closed in two layers without tension. Drains were not used in any case. The harvested dermofat graft was then soaked in normal saline.
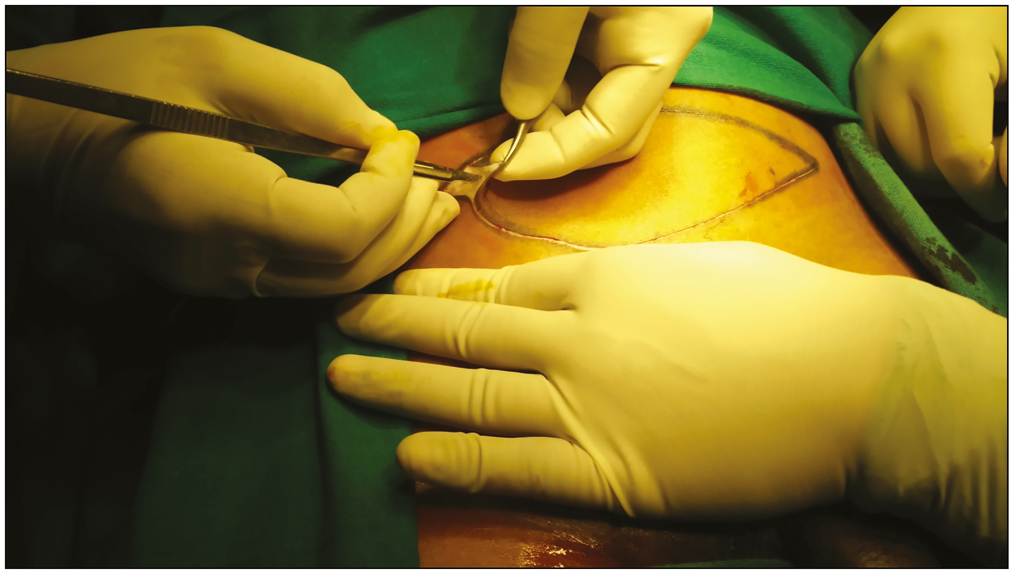
- De-epithelialization of dermofat graft being performed
Attention was then directed to the penis. A simple rubber catheter was inserted into the penis. A subcoronal incision was then made after injecting a small amount of normal saline to outline the subdartos space, and this incision was of two types: in the first, it was circumferential and included cutting the frenulum and in the second type it stopped at the frenulum. Frenulotomy was performed in patients who had a tight frenulum with patients complaining of tightness during erection.
The penile skin along with the dartos was then dissected off the penile shaft by dissection in the subdartos space, which is relatively avascular. Dissection was carried on till the root of the penis and beyond to create a space for accommodating the dermofat graft. The dermofat graft was then laid on top of the penile shaft and secured to Buck’s fascia using 3-0 polyglactin sutures. Care was taken not to insert sutures overlying the dorsal neurovascular bundles of the penis which were clearly visible on either side. The dermofat graft was attached circumferentially ending on either side of the urethra which was spared. Following this, the dermofat graft was sutured to the proximal penile shaft using multiple sutures, but the proximal end which was tunneled beyond the penile root was not attached so that it could glide freely during erection [Figure 2]. The penile skin was then rolled back to its original location and secured to the original incision site using 4-0 polyglactin sutures [Figure 3].

- Dermofat graft attached to penis

- Appearance at the end of surgery with penile skin replaced back to its original position
Post-operatively, light dressings were applied over the operated areas and patients were given a course of oral antibiotics and analgesics were given liberally. They were instructed not to attempt erections for 2 weeks following surgery, but no anti-erection medications were given. They were asked to attend the next day for catheter removal. Stitches for the donor area were removed around 10 days after surgery.
Technique of SEPA flap
The SEPA flap was marked out on the right side extending from the umbilicus to the root of the penis in a vertical fashion [Figure 4]. The width of the flap was designed according to the penile girth excluding the urethra. The same process of anesthesia, as was used during dermofat graft harvesting, was used here and following that de-epithelialization was done extending from the tip of the flap to the penile base such that the flap would easily reach the coronal sulcus. The flap was elevated at the level of the superficial fascia near the umbilicus, and the depth was progressively increased such that near the root of the penis the dissection was deep to the Scarpa’s fascia so as to protect the vascular pedicle [Figure 5].
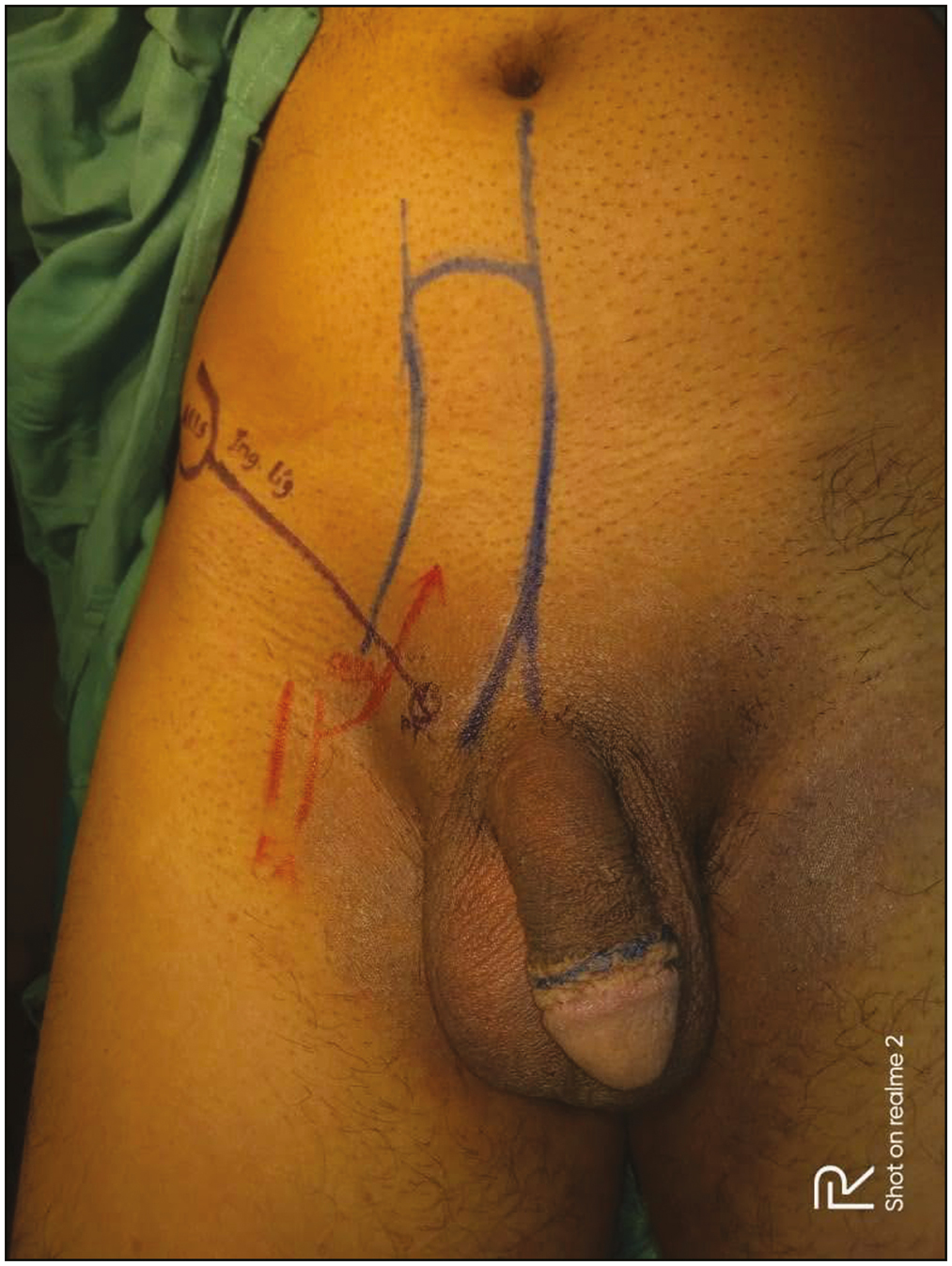
- Marking of SEPA flap
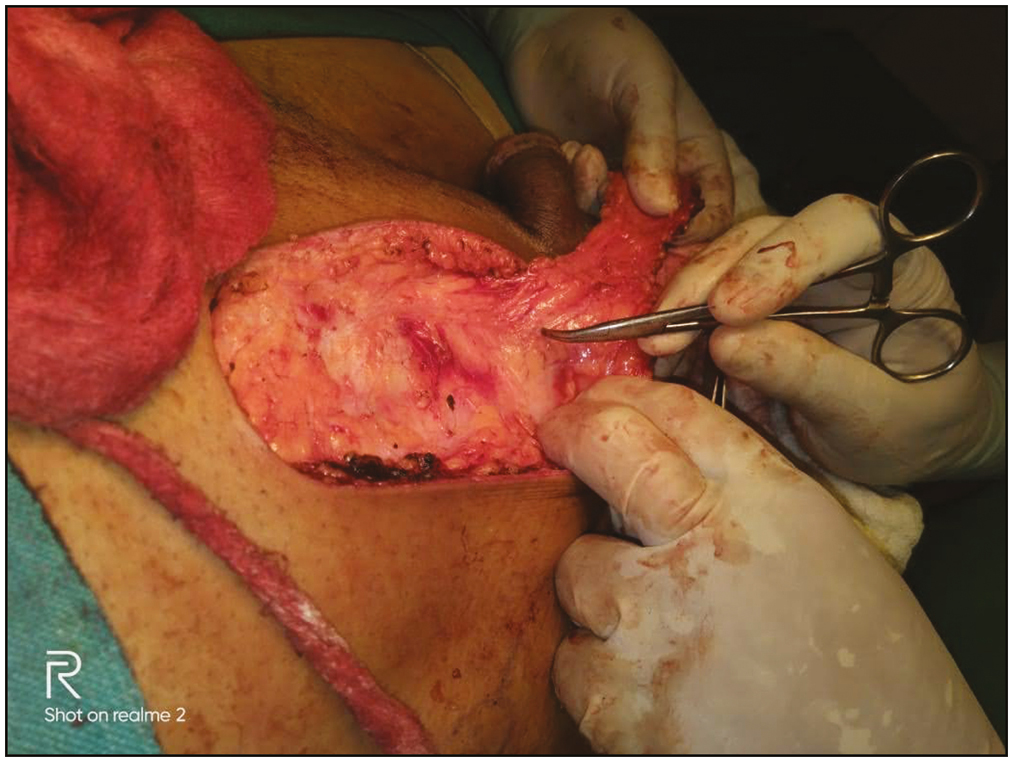
- he pedicle of the SEPA flap
An incision was then made proximal to the coronal sulcus and dissection performed in the subdartos space, and the dissection was continued till the base of the flap such that the flap could be easily tunneled into the penis. The de-epithelialized SEPA flap was then anchored to the penis as described before.
Post-operative instructions were similar as in dermofat grafting.
RESULTS
Ten patients were operated in total for penile girth augmentation, six of them undergoing dermofat grafting and four patients the SEPA flap. The age range of patients was 24–57 years. It was observed that all patients had a penile girth which was within the normal range of the population.[11]
Two patients in the SEPA group had complications following surgery and three patients in the dermofat graft group encountered complications; therefore, the total complication rate was 50%.
One patient in the SEPA group who had simultaneous ligament surgery had a 1 cm2 area of skin loss over the dorsal surface of the penile shaft with exudation of liquid fat which was managed conservatively with dressings and the area healed after 17 days. The second patient with SEPA flap had obstruction of his urinary outlet from severe swelling of the foreskin with loss of around 3 cm2 of dorsal skin over penile shaft with urine tracking through this aperture. He was managed with catheterization and dorsal slit of the prepuce and debridement of the necrotic area, following which dressings were done on a regular basis with Cadexomer iodine. The catheter was removed after 7 days and the area got epithelialized after 1 month of dressing.
One patient in the dermofat group had partial necrosis of the inner foreskin which was managed with debridement and primary closure and the area healed thereof. Two patients had swellings in their penile shafts with collection of liquid fat which then burst out spontaneously. Conservative management was advocated with regular dressings and the areas healed in 2–3 weeks’ time.
A slight decrease of penile girth was noted by all patients compared with the immediate post-operative period [Figure 6], which was natural as some degree of fat absorption usually occurs [Figure 7].

- Pre- and post-operative pictures of dermofat graft (upper) and SEPA flap (lower)
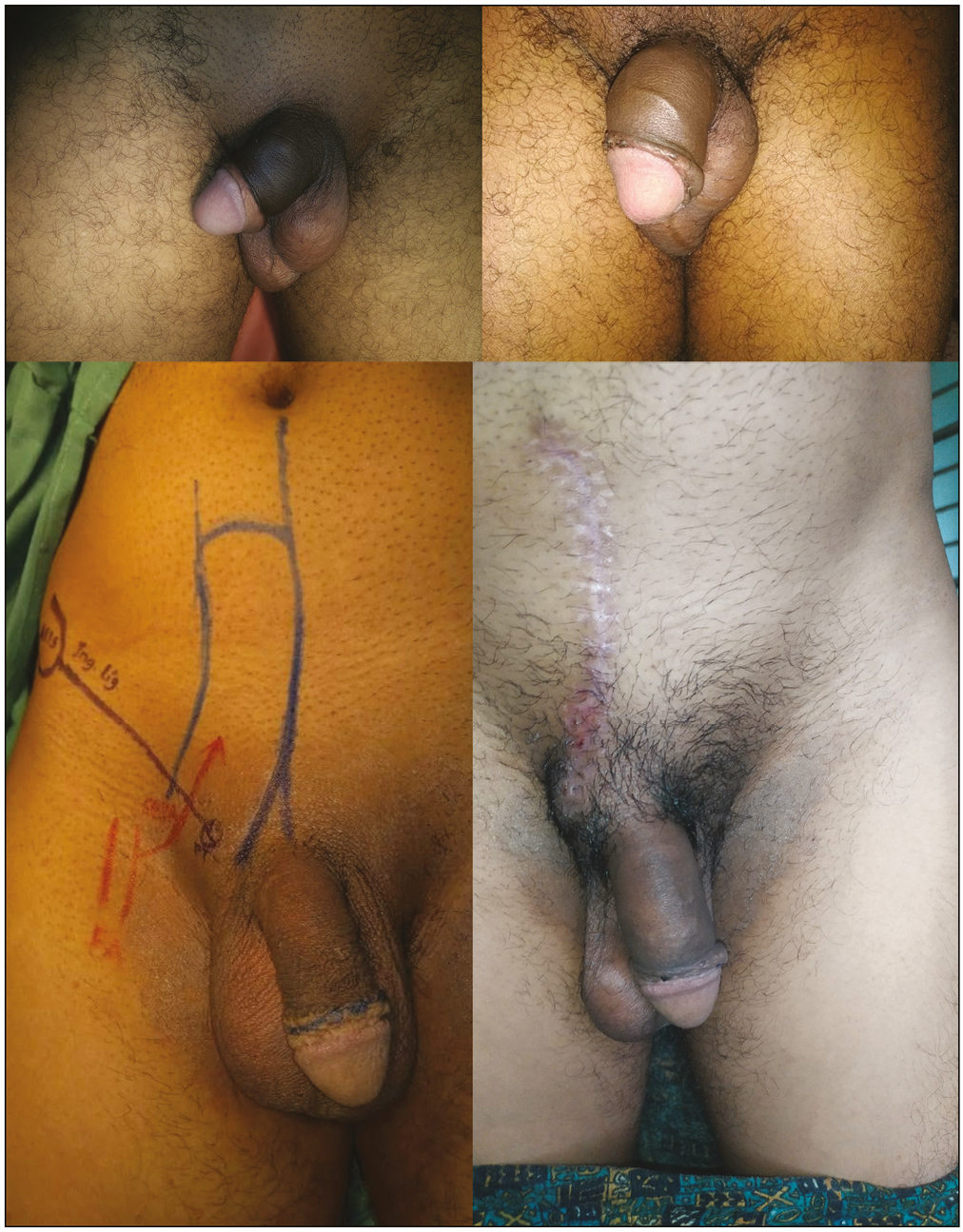
- Pictures of dermofat grafting done in a case of previous fat injections to penis (upper) and SEPA flap augmentation of penis (lower)
With regard to surgery using dermofat, the mean circumference of patients pre-operatively was 9.8 with a variance of 0.788 and a standard deviation of 0.887. The mean circumference of patients in the post-operative period was 11.85 (difference in mean between pre- and post-operative measurements was 2.05) with a variance of 0.803 and a standard deviation of 0.896. The t-value was -3.98 and the P-value was 0.001298 with the result being significant at P < 0.05.
In the SEPA group, the pre-operative mean was 9.9 with a variance of 2.6 and a standard deviation of 1.61. The post-operative mean was 12 (difference in mean between pre- and post-operative measurements was 2.1) with a variance of 2.16 and a standard deviation of 1.47.
The t-value was 1.92 and the P-value was 0.05 with the result not significant at P < 0.05.
The post-operative APPSSI score ranged from 2 to 12 with one patient extremely dissatisfied with the surgical outcome and one patient reporting no benefit from surgery.
Additional observation was that complications were most frequent in patients who had intact foreskin compared with those who were circumcised.
DISCUSSION
Patients who desire penis augmentation surgery feel that they have a thin penis and would be unable to satisfy their sexual partners; therefore, a psychosexual assessment is recommended in them.[12] The objectives of a penis girth augmentation surgery are increase of penile girth permanently without impairing penile sensations or erections. The consistency of the penis should be normal following augmentation, and the appearance should be aesthetic. A lot of procedures have evolved over the years ranging from minimally invasive injection therapies to extensive surgical procedures but none has been accepted as the “gold standard” with regard to permanent penile girth augmentation.
Patients need to be assessed first whether they are suitable candidates for penile girth augmentation. Many of these have unrealistic expectations and are especially difficult to counsel. These patients may turn aggressive if they do not get their needs fulfilled after surgery and surgery is best avoided in them. The APPSSI score may be useful in choosing patients for surgery.[13] Patients need to be intensively counseled that penile girth augmentation is a procedure which might have a lot of complications and one must be ready to accept these.[14] The penile girth needs to be measured and compared with the population as most of these patients have a normal penile girth which they do not know of.
Published literature is few with regard to penile girth augmentation, although it has been mentioned that the likelihood of complications with these procedures is quite high. The complication rate has probably been underreported in studies. With regard to girth augmentation using subcutaneous fat injections, the American Urological Association does not consider it to be procedure, which is safe and at the same time efficacious.[15] The International Society for Sexual Medicine has emphasized that girth augmentation can have serious complications which patients need to be apprised of before undergoing these procedures.[16]
There are a variety of procedures available when penile girth augmentation is done by invasive surgery. These employ human and porcine acellular dermal matrix, allografts, dermofat grafts, and SEPA flap, among others.[17181920] Allografts are technically easier to use as they avoid donor site morbidity and scars but the negative point against their use is their cost which might be a problem in patients of developing countries. Also, how long the allografts are going to last is not standardized. Therefore, autografts and flaps are used for penile augmentation in many patients.
The SEPA flap has been used in penile reconstruction, although the design was different.[20] In this series, the SEPA flap was designed according to the outline provided by Dias[21] with the superior extent of the flap extending to the umbilicus and the inferior extent reaching to the pubic tubercle and staying around 2.5 cm away from it. Since the flap is narrow, the donor site can be closed primarily. Anatomical studies have shown that the vessel lies just superficial to Scarpa’s fascia where it crosses the spermatic cord and then becomes more superficial as it ascends upward toward the umbilicus. Thus, the flap can be raised between the superficial and deep layers of fat near the umbilicus and the depth progressively increased as one approaches the pubic tubercle. The de-epithelialized flap can be rotated 180° to be inserted into the penis and providing augmentation to it.
Autologous dermis has been used for penile augmentation with good results.[18] However, inclusion of a thin layer of fat along with the dermis to create a dermofat graft can actually increase the degree of augmentation more. It needs mention here that a thicker layer of fat led to complications in our patients as much of it was seen to be liquefied and collected at the root of the penis; therefore, caution must be exercised in patients who desire “excessive girth augmentation.”
CONCLUSION
To conclude, penis girth augmentation using SEPA flaps and dermofat grafts is indicated in patients who fulfill the criteria and give appreciable girth increase, but patients need to be informed of the potential complications of these surgeries and they must be ready to accept those. Only moderate girth increase is recommended to decrease the stress on the overlying penile skin. Studies with larger patient groups are needed to standardize these procedures. It is also recommended to follow-up these patients for longer periods to find out the long-term results of surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
The author declares no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
- Sociocultural influences on men’s penis size perceptions and decisions to undergo penile augmentation: A qualitative study. Aesthet Surg J. 2019;39:1253-9.
- [Google Scholar]
- Penile length is normal in most men seeking penile lengthening procedures. Int J Impot Res. 2002;14:283-6.
- [Google Scholar]
- The effects of penile girth enhancement using injectable hyaluronic acid gel, a filler. J Sex Med. 2011;8:3407-13.
- [Google Scholar]
- Short-term results of incremental penile girth enhancement using liquid injectable silicone: Words of praise for a change. Asian J Androl. 2007;9:408-13.
- [Google Scholar]
- Efficacy and safety of penile girth enhancement by autologous fat injection for patients with thin penises. Aesthetic Plast Surg. 2012;36:813-8.
- [Google Scholar]
- The advancement of pure local anesthesia for penile surgeries: Can an outpatient basis be sustainable? J Androl. 2007;28:200-5.
- [Google Scholar]
- Using a dermis fat graft for volumetric rejuvenation of deep superior sulcus in the eyelid due to an anophthalmic socket. Eur Arch Med Res. 2021;37:192-4.
- [Google Scholar]
- Superior sulcus volumetric rejuvenation utilizing dermis fat grafting. Aesthet Surg J. 2015;35:892-8.
- [Google Scholar]
- Penile girth enhancement procedures for aesthetic purposes. Int J Impot Res. 2022;34:337-42.
- [Google Scholar]
- Augmentation phalloplasty patient selection and satisfaction inventory: A novel questionnaire to evaluate patients considered for augmentation phalloplasty surgery because of penile dysmorphophobia. Urology. 2007;70:221-6.
- [Google Scholar]
- Complications and management of penile girth enhancement with acellular dermal matrix. J Sex Med. 2019;16:2011-7.
- [Google Scholar]
- 2018. Penile augmentation surgery. Available from: https://www.auanet.org//about-us/policy-and-position-statements/penile-augmentation-surgery. [Last accessed on 2022 Aug 12]
- 2019. Penis enlargement surgery: Men should know about complications. Available from: https://www.issm.info/news/sex-health-headlines/penis-enlargement-surgery-men-should-know-about-complications/. [Last accessed on 2022 Aug 12]
- Original technique for penile girth augmentation through porcine dermal acellular grafts: Results in a 69-patient series. J Sex Med. 2012;9:1945-53.
- [Google Scholar]
- Autologous dermal graft combined with a modified degloving procedure for penile augmentation in young adults: A preliminary study. Andrology. 2016;4:927-31.
- [Google Scholar]
- Cosmetic penile enhancement surgery: A 3-year single-centre retrospective clinical evaluation of 355 cases. Sci Rep. 2019;9:6323.
- [Google Scholar]
- Reconstruction of a circumferential penile shaft defect using bilateral superficial external pudendal artery perforator flaps. Arch Hand Microsurg. 2018;23:296-300.
- [Google Scholar]
- The superficial external pudendal artery (SEPA) axial-pattern flap. Br J Plast Surg. 1984;37:256-61.
- [Google Scholar]




