
Translate this page into:
Esthetic and reconstructive options for earlobe deformities

*Corresponding author: Uwe Wollina, Former Head of Department of Dermatology and Allergology, Städtisches Klinikum Dresden, Dresden, Germany. uwollina@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Wollina U, Goldman A, Machado Luz P, Guindani Marson V. Esthetic and reconstructive options for earlobe deformities. J Cutan Aesthet Surg. 2025;18:7-15. doi: 10.25259/JCAS_122_2024
Abstract
Background:
The earlobe plays a significant role in framing the face and complementing the appearance of earrings, hairstyles, and other facial features. In addition to the growth of the earlobes with the aging process, other changes can compromise the shape, size, and overall youthful appearance of this region. The main changes are evidenced by the elongation and ptosis of the earlobes, loss, atrophy of soft tissues, and formation of wrinkles in addition to deformities produced by surgical procedures, placement of earrings, and piercings or earlobe gauging.
Objective:
The authors describe the main changes in the earlobes and review the current treatment modality for earlobe rejuvenation and reconstruction, addressing the anatomy, common esthetic concerns, and various therapeutic approaches.
Methods:
A narrative review of treatment options was performed. We searched PubMed databases. Based on the diagnosis of changes, less invasive surgical procedures, use of laser, and fillers with fat or hyaluronic acid represent therapeutic options.
Results:
Significant improvement of the senile earlobe and correction of anatomical and esthetic deformities can be attenuated or corrected through different approaches. Proper diagnosis of the changes will determine the best treatment or even the combination of procedures.
Conclusion:
Surgical procedures, laser rejuvenation, fat injection, and fillers represent simple and effective options for treating esthetic problems and acquired deformities of the earlobes.
Keywords
Atrophy
Esthetics
Hyaluronic acid
Lasers
Rejuvenation

INTRODUCTION
Earlobes play an important role in facial esthetics. In general, young people present a good position, adequate shape, and pleasant appearance. The use of adornments, such as earrings, supports the earlobes with an area of esthetic prominence. Age, gender, culture, ethnicity, and fashion affect the esthetic ideal.1,2
The aging process, its characteristics, and changes in the human body also affect the earlobes. Located in a plane perpendicular to the face, ideally, the lobes should be elastic and have a good volume that does not indicate sagging. The deflation or emptying of these structures, as well as their ptosis and stretching, reflect esthetically unpleasant signs.3
The deflated and flaccid appearance of the earlobes with loss of their elastic capacity, position, and size compromises facial esthetics and must be observed in facial rejuvenation procedures. Ptosis and elongation of the lobes are the most obvious signs of aging in this anatomical area, leading to an unattractive appearance. In addition to congenital deformities, the main acquired changes related to earlobes are produced by trauma, placement of earrings and adornments, and surgery.4 One study showed that the length of the lobes increases by 30–35% from the age of 30 to the age of 60.5
Treatments for earlobe changes depend fundamentally on the causes and appearance of the deformities. Options can be non-surgical with fat or filler injection or surgical with soft-tissue remodeling. The earlobe contains no cartilage. As a result of the natural aging process, the combination of persistent gravitational forces and a decline in tissue elasticity leads to ptosis and wrinkling.6
According to Alexander, earlobe ptosis is defined as a lobe >25% of the total length of the ear. The normal length of the earlobes (distance from the antitragus to the lower edge of the ear) is between 1.5 cm and 2.5 cm in children and adults.7
ANATOMY OF THE EARLOBE
The earlobe (lobulus auriculae) is the inferior portion of the external ear and consists predominantly of soft tissues, including areolar connective tissue and adipose tissue, which provide its flexible and pliable nature. The areolar tissue contains a matrix of collagen and elastin fibers that provide structural support and flexibility. Adipose tissue enhances the softness and pliability of the earlobe while also serving as an energy reserve. Unlike the rest of the auricle, the earlobe lacks cartilage, contributing to its distinct flexibility.
Due to its rich vascular and nerve supply, the earlobe can play a role in thermoregulation and sensory perception. The arterial supply comes from branches of the posterior auricular artery, the superficial temporal artery, and branches of the external carotid artery. Venous vessels drain into the external jugular vein. The great auricular nerve, a branch of the cervical plexus, mainly provides the sensory innervation of the earlobe. The auriculotemporal nerve extends some fibers into the earlobe.8,9
There are two major types of earlobe morphology – attached and pendulous. The pendulous type can be further classified into acute angled earlobes (Type A), right-angled earlobes (Type B), and obtuse-angled earlobes (Type C).10 Another classification includes four types of earlobes: arched, tongue-shaped, square, and triangular.11
AGE-RELATED CHANGES AND ESTHETIC ASPECTS
As earlobes age, they undergo several esthetic changes. A common feature is volume loss, where a reduction in adipose and connective tissue leads to a deflated or atrophic appearance. This is often accompanied by sagging and lengthening of the earlobes, particularly in individuals who have worn heavy earrings.12 In addition, aging results in the development of wrinkles and creases on the earlobe surface. Torn or enlarged earlobe holes are common earlobe changes. Skin texture changes such as roughness or irregularity may develop by photodamage.13
Deformities of the earlobes, whether associated with aging or not, can represent an esthetic concern. Numerous surgical and non-surgical modalities aim to enhance the appearance, texture, shape, deformities, and size of these structures. Hence, the importance of the surgeon’s knowledge of the various reconstructive options cannot be underestimated. Sometimes, the combination of more than one procedure can bring benefits to the repair process. Individualized treatment based on a precise diagnosis of the alterations yields effective, safe, natural, and anatomical results for the earlobes.
METHODS
Since the earlobes play an important role in facial esthetics, this manuscript aims to demonstrate, in a didactic and objective manner, the different surgical options for each type of existing deformity.
We have completed a narrative review on treatment options on PUBMED©. A systematic review was not feasible due to the high heterogeneity of articles on this topic. The focus of this review is on traumatic ear lobe loss, pixie ear, earlobe ptosis, and correction of earlobes after gauging. Articles referring to traumatic, congenital, and acquired cleft deformities were excluded. Articles on earlobe keloid treatment were also excluded. Key terms in the search included “earlobe AND reconstruction” and “earlobe AND rejuvenation.” Languages included were English, Spanish, Portuguese, and German. The considered articles were published between 2000 and 2024. We obtained 359 hits for “earlobe reconstruction” and 21 hits for “earlobe rejuvenation.” We searched the reference lists of relevant articles and added seven more articles. We included case reports (n = 11), case series (n = 9), reviews (n = 4), and uncontrolled trials (n = 4).
We noted limitations since no randomized controlled trials were available. Most case series had single-digit numbers of patients. Not all publications provided data for both earlobes and/or earlobe symmetry.
TREATMENT OPTIONS FOR EARLOBE REJUVENATION
Minimal invasive methods
A variety of non-surgical and surgical treatment options are available for addressing the esthetic aspect and deformities of the earlobe. Dermal fillers are frequently used to restore volume and rejuvenate deflated earlobes. The main fillers are hyaluronic acid (HA), calcium hydroxylapatite, and polyL-lactic acid. For the earlobes, HA fillers are preferred for Mowlavi Grade I and II patients. Results are immediately visible after injection, as the volume is restored, improving the fullness, laxity, and wrinkles [Figure 1]. HA fillers also restore impaired protective skin barrier function. Fillers provide a temporary improvement, lasting up to 14 months. Risks associated with the treatment are usually mild, including potential swelling, bruising, or infection at the injection site.14-16
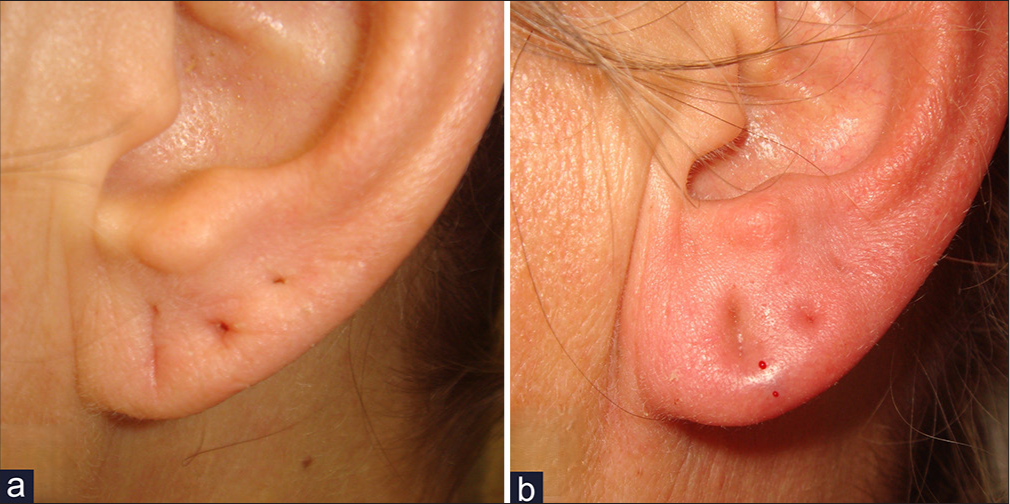
- (a, b) A 46-year-old female patient with loss of volume and fine wrinkling of the ear lobe. Rejuvenation with hyaluronic acid filler treatment. (a) Before treatment. (b) After filler injection reduced wrinkling and increased fullness.
Fat grafting or autologous fat transfer is an alternative method for restoring volume to aging or deflated earlobes. Usually, fat grafting provides safe results since it uses the patient’s tissue, minimizing the risk of allergic reactions. The method increases earlobe volume and decreases fine wrinkles and creases [Figure 2]. The results are often long-lasting compared to dermal fillers. Fat resorption should be considered. Risks include potential fat infection or hypercorrection. In some cases, multiple sessions may be needed to achieve optimal results.17,18

- (a) Atrophic and wrinkled earlobe. (b) Fat grafting into the earlobe during rhytidoplasty. (c) Result 3 months after the procedure.
Fat injection and fillers are effective, minimally invasive techniques for restoring earlobe volume and enhancing a youthful appearance. Fat transfer uses autologous fat harvested from donor sites such as the abdomen, thighs, or submental region, which is processed and injected in small amounts into the central body, medial, and lateral edges of the earlobe. This approach provides natural, long-lasting results, improves skin quality through adipose-derived stem cells, and is ideal for addressing atrophy, elongation, and trauma-related volume loss.
Fillers, such as HA, offer immediately for mild-to-moderate volume loss, wrinkles, and soft-tissue atrophy. Injection points include the central body, peripheral margins, and areas around stretched piercing holes. HA is safe, while alternatives such as calcium hydroxylapatite or poly-L-lactic acid provide longer-lasting effects.
Both techniques require precise placement using small-gauge cannulas or needles to prevent lumps or asymmetry. Fat injections have greater longevity but may need multiple sessions, while fillers typically last 6–12 months. Younger patients may benefit more from fillers, while fat transfer suits those with significant volume loss. Patient selection and careful technique represent important cars to achieve natural results.
Earlobe repair surgery
Earlobe repair surgery is the most effective treatment for individuals with torn, split, or stretched earlobe holes and after traumatic loss of the earlobe [Figures 3 and 4]. These procedures can close large or torn piercings, restore the natural contour of the earlobe, and correct overly elongated lobes. For patients with Mowlavi stages III and IV earlobe ptosis, surgery is the only solution. The existing deformity or deformities determine the best surgical procedure.19,20
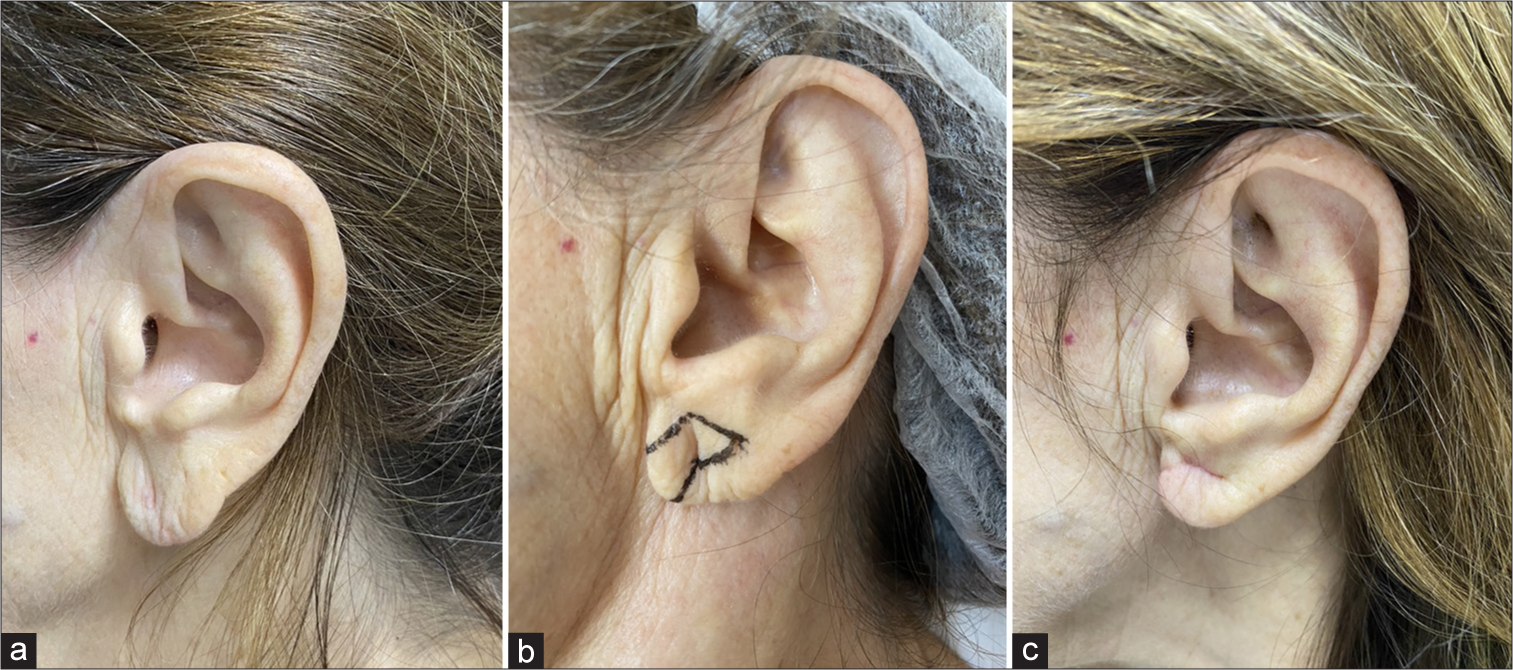
- (a) A 61-year-old patient with ptosis and stretching of the earlobe. (b) Surgical planning. (c) Result 1 month after surgical procedure.

- (a) Elongated earlobe in a 72-year-old patient. (b) Planning of surgical resection and reconstruction flaps. (c) One month postoperatively with esthetic improvement.
For earlobe ptosis, it is essential to remove excessive tissue but obviate earlobe deformity. In case of severe ptosis, the sub-antitragal groove technique aims to preserve the lateral edge of the ear lobule and minimize the risk of free-border notching.21 In case of an attached, tapered, and low-set earlobe (pixie ear), infraauricular skin re-draping is suitable. From the frontal view, no scar is visible, and the earlobe size is preserved.22 For protruding earlobes, a modified fish-tail excision on the posterior site is an option.23
For earlobe reconstruction, various techniques are available [Table 1]. Two-stage procedures include the Zenteno Alanis technique with an infraauricular vertical flap,24 the modified Limberg flap,25 the preauricular flap,26 and the posterior-based interpolation flap with the addition of a double Z-plasty.27
Due to a lesser downtime, one-stage procedures have gained increasing interest, such as the superiorly based preauricular transposition flap,28 the inferior pedicle flap,29 the freestyle perforator-flap surgery (Doppler-sonography is crucial for flap design),30 and a combination of two rotation flaps, one from the lower auricle and the other from the infraauricular area with a V–Y advancement flap closure of the donor defect.31 A commonly used surgical technique is the modified bilobed Gavello flap, which is achieved by elevating a bilobed flap horizontally below the earlobe defect and then folding the two flap lobes together.24,32 Another option for a single-stage procedure is the combined preauricular, retro auricular bilobed flap for earlobe reconstruction when various esthetic units are involved.33
| Technique | Indication (s) | Advantages | Limitations |
|---|---|---|---|
| Modified fish-tail flap | Protruding earlobe | Achieves adjustable vertical height & sufficient correction through asymmetric oblique suturation with minimal skin excision and reduced risk of keloids, good esthetic outcome. | Might need dog-ear excision. |
| Infraauricular skin redraping method | Pixie ear | One-stage reconstruction, simple and easy to perform, natural appearance of the earlobe, tension-free; the retroauricular scar is inconspicuous from frontal view. | None known. |
| Zenteno Alanis technique | Traumatic loss of earlobe | Two-stage procedure with an infraauricular vertical flap, good esthetic outcome. | Division of the flap 3 weeks after primary surgery. |
| Gavello technique | Traumatic loss of earlobe | Single-stage procedure with a horizontal bilobed flap on postauricular mastoid skin, acceptable esthetic outcome. | Some risk of hypertrophic scarring. |
| Doubled-over Limberg flap | Traumatic loss of earlobe | Two-stage procedure, no shrinkage, minimal necrosis, good esthetic outcome. | Needs defatting after 3–4 months. |
| Preauricular flap | Traumatic loss of earlobe | Two-stage procedure, simple technique, good esthetic outcome. | Second step after formation of the folded flap 6 months later |
| Superiorly based preauricular transposition flap | Traumatic loss of earlobe | Single-stage procedure, technically simple and safe, satisfying esthetic outcome. | May narrow the auriculotemporal sulcus. |
| Posterior-based interpolation flap with the addition of a double Z-plasty | Traumatic loss of earlobe | Two-stage procedure for defects of several esthetic units, acceptable esthetic outcome. | Needs a revision after 4 weeks for pedicles and cicatricial contour by V-Y plasty. |
| Posterior auricle bilobed cartilage-skin flap | Traumatic loss of earlobe | Single-stage minimal invasive surgery; cartilage harvested from the same region; it can reconstruct a relatively large earlobe with a natural shape; recreates the otobasion inferius-to-subaurale distance seen in the contralateral ear, good esthetic outcome | There is a risk of bulky reconstructed earlobe, harvesting the first flap generates a narrow auriculotemporal sulcus. |
| Combined preauricular, retroauricular bilobed flap | Traumatic loss of earlobe | Single-stage, easy to perform, acceptable esthetic outcome. | None known. |
| Freestyle perforator flap | Traumatic loss of earlobe | One-stage reconstruction which provides more flexibility in selecting the donor site, esthetic outcome. | Pre-surgical Doppler-ultrasound is necessary. |
| Anteriorly based post-auricular flap | Traumatic loss of earlobe | One-stage procedure also for larger defects, acceptable esthetic outcome. | Hematoma. Risk of damage of sensory nerves of the earlobe. |
| V to Y advancement flap | Small lobular defects after surgery | One-stage procedure, well-vascularized flap, minimal risks, and good esthetic outcome. | Not for larger defects. |
| Double opposing perpendicular linear repair | Dilated ear lobules after gauge ear piercing | One-stage procedure, easy to perform, dog-ears are avoided, does not violate the thin inferior rim of the lobule, prevents notching, good esthetic outcome | None known. |
| Local flap technique by Williams and Majumder34 | Dilated ear lobules after gauge ear piercing | One-stage procedure, local flap, uncomplicated, good esthetic outcome. | Creating an earlobe slightly smaller and flatter than it was before gauge ear piercing, imprecise cuts could lead to suboptimal reconstruction. |
| Local flap technique of Henderson and Malata35 | Dilated ear lobules after gauge ear piercing | One-stage procedure, easy, good esthetic outcome. | Insufficient tissue may lead to a small lobule with a flat appearance. |
| Wedge excision according to De la Sotta et al.36 | Dilated ear lobules after gauge ear piercing | One-stage procedure, minimal excisions, good esthetic outcome. | Requires sufficiently thick tissue on the rims of the lobule. |
| Double opposing perpendicular linear closure | Dilated ear lobules after gauge ear piercing | One-stage procedure even for larger defects, good esthetic outcome, dog-ear formation is avoided, prevents notching. | None known. |
Reconstruction of earlobe defects after gauging (flesh tunnel) can be challenging [Figure 5]. One technique uses the removal of the inferior portion of the dilated earlobe and repair of the hole by de-epithelialization of the margin. This is followed by a subsequent approximation of the remaining earlobe. The technique results in a slightly smaller and flatter earlobe compared to gauge.34 A related technique removes the excess tissue from the anterior half of the defect. The remaining posterior flap is de-epithelialized and sutured to the superior rim in an L-shaped pattern.35

- 34-year-old patient, who has been using (a) earlobe gauging (rings) for 20 years. (b) Preparation of a local flap, de-epithelization of the inner rim of the hole. (c) Flap positioned and sutured. (d) Result 1 month after surgery (Henderson-Malata technique).
For patients with thick tissue on the rims of the lobule, it is possible to create 3 wedge excisions around the rim of the dilated lobule, followed by an approximation of these wedges with anterior and posterior sutures.36 Another option is a double opposing perpendicular linear repair. The inner circle of the defect is undermined by fat. A linear closure is then placed on the anterior aspect of the circular lobular defect, followed by a linear closure on the posterior site at a 90° angle. This results in a natural appearance with minimal scarring.37 In most patients, surgical repair provides a permanent solution with minimal risk of complications.
Multiple and creative technical options involving flaps and mobilization of soft tissues, support the surgical option in correcting earlobe deformities. Risks include infection, scarring, or asymmetry.38-45
De-epithelization and healing techniques
De-epithelization procedures are essential for treating various earlobe deformities and rejuvenating the region. These techniques involve removing the epithelial layer to promote healing and tissue remodeling. Some de-epithelization techniques are as follows:
Trichloroacetic acid (TCA)
TCA peels are chemical agents used to resurface the skin and stimulate collagen production. They are effective for mild surface irregularities and wrinkles, helping improve the texture and appearance of the earlobe. However, precise application is critical to avoid overexposure, which may lead to burns or scarring.46
Phenol peels
Phenol peels are deeper chemical agents compared to TCA, useful for more significant skin damage. They achieve profound resurfacing, but their use is limited due to a higher risk of complications, including hypopigmentation and prolonged healing.47
Radiofrequency (RF)
RF devices offer controlled heating of the skin, leading to collagen contraction and regeneration. Useful for mild laxity and rejuvenation, RF is minimally invasive but less effective for severe deformities.48
Carbon dioxide (CO2) and erbium-yttrium aluminum garnet (YAG) laser
Fractional or ablative CO2 and/or erbium-YAG lasers effectively target deep wrinkles and improve skin laxity by stimulating collagen. They allow precise control of tissue removal and are excellent for earlobe rejuvenation with faster recovery compared to traditional methods.49
Healing techniques are also useful tools for earlobe deformities treatment.50 Some examples of these options are as follows:
Glue (tissue adhesives)
Glue provides a non-invasive method for wound closure, reducing scarring and the need for sutures. Ideal for smaller wounds or less invasive procedures but may not provide the tensile strength required for larger repairs.
Steristrip
These adhesive strips offer a simple and cost-effective method for superficial wound closure. Steristrips are less durable than sutures or staples and may not be ideal for high-tension areas.
Suturing
Suturing remains the gold standard for securing de-epithelialized areas. It provides optimal wound approximation, strength, and control over esthetic outcomes. Absorbable sutures are often preferred to reduce follow-up interventions.
In earlobe reconstruction, sutures are selected based on the defect’s size and location. Non-absorbable sutures (e.g., Nylon and Prolene) are used for precise external skin closure, while absorbable sutures (e.g., Vicryl and Monocryl) support deeper layers without removal. Monofilament sutures reduce infection risk and techniques such as interrupted or running sutures manage tension and closure efficiency. The surgeon’s choice ensures optimal healing and esthetic results.
Stapler techniques
Surgical staplers offer a quick and efficient closure method, but they may be less precise for smaller or highly esthetic areas like the earlobe. Staplers are more suitable for large-scale closures rather than delicate, visible regions. Usually, this kind of suture is expensive.
The choice of de-epithelization and healing techniques depends on the degree of deformity, patient preferences, and the desired esthetic outcome. For minimal rejuvenation, non-invasive methods such as TCA or RF are preferred. For more significant changes, CO2 laser or suturing may yield better results. Healing methods should focus on minimizing scarring and achieving natural contours, with suturing being the most versatile for achieving precise results.50
Combining techniques, such as using RF with sutures or TCA with tissue adhesives, may enhance outcomes for certain cases. However, careful patient selection and thorough counseling about potential risks and benefits are crucial for success.
DISCUSSION
Acquired or non-acquired earlobe deformities can lead to esthetic impairment. Deflation, ptosis, loss of volume, and changes in skin texture and quality are the main changes found in this region. The most frequent acquired deformity from aging involves elongation or ptosis of the earlobe. Loss of elastic fibers and a consequent gravitational pull contribute to this deformity. Reconstruction considers the type of deformity, remaining tissues, scars, and characteristics such as shape, size, and volume of the lobes. The aging process, intrinsic and extrinsic causes, and trauma or adornment are the main factors related to changes in these structures. It is not uncommon for sagging and facial and cervical aging to be accompanied by esthetic changes to the earlobes. Studies showing patients’ opinions on the esthetic standards of the ear revealed that the helix and earlobe were the structures people found most concerning. Notable differences emerged between genders, with educational background also playing a role in these concerns.51
Mowlavi et al. proposed a classification system for earlobe ptosis. This classification aims to enhance the precision of earlobe reduction or reconstruction treatments.3 Correction or improvement of these unsightly characteristics must seek a harmonious result, restoring and respecting the proportional dimensions of the lobe with the ear, its volume, texture, and position.
Numerous types of surgical and non-surgical treatments are described for rejuvenating earlobe changes. Treatment must be based on the anatomical changes present and seek a global esthetic improvement in this region.41,52
There is good evidence that HA fillers improve mild earlobe ptosis, but severe ptosis may require surgery.14,19 Fat transfer is effective in volumizing and reduction of creases and wrinkles in earlobe rejuvenation. The results are less predictable but often last longer than fillers.17
Removal of excess tissue and the use of triangular flaps to correct elongated earlobes, minimizing scar represents an option for earlobe reconstruction.40
In general, a period of 2–3 months is allowed before placing a new piercing after reconstruction of earlobe deformities. This period varies according to the type of deformity, technique used, and, mainly, the recovery and healing process of each patient. A new hole should be avoided over the scarred area to minimize the risk of the problem recurring.
CONCLUSION
Deformities of the earlobes, whether associated with aging or not, can represent an esthetic concern. Numerous surgical and non-surgical modalities aim to enhance the appearance, texture, shape, deformities, and size of these structures. Individualized treatment based on a precise diagnosis of the alterations yields effective, safe, natural, and anatomical results for the earlobes.
Authors’ contributions
All authors have contributed equally.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Anthropometric study of human ear: A baseline data for ear reconstruction. J Craniofac Surg. 2022;33:1245-9.
- [CrossRef] [PubMed] [Google Scholar]
- 3D assessment of ear morphology. J Oral Biol Craniofac Res. 2023;13:622-9.
- [CrossRef] [PubMed] [Google Scholar]
- The aesthetic earlobe: Classification of lobule ptosis on the basis of a survey of North American Caucasians. Plast Reconstr Surg. 2003;112:266-72.
- [CrossRef] [PubMed] [Google Scholar]
- A morphometric study of the newborn ear and an analysis of factors related to congenital auricular deformities. Plast Reconstr Surg. 2017;140:147-55.
- [CrossRef] [PubMed] [Google Scholar]
- Morphometry of the adult human earlobe: A study of 547 subjects and clinical application. Plast Reconstr Surg. 2003;111:2398-402.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of earlobe ptosis and pseudoptosis in patients seeking facial rejuvenation surgery and effects of aging. Plast Reconstr Surg. 2004;113:712-7.
- [CrossRef] [PubMed] [Google Scholar]
- A morphometric study of the human ear. J Plast Reconstr Aesthet Surg. 2011;64:41-7.
- [CrossRef] [PubMed] [Google Scholar]
- The arterial blood supply of the helical rim and the earlobe-based advancement flap (ELBAF): A new strategy for reconstructions of helical rim defects. J Plast Reconstr Aesthet Surg. 2015;68:56-62.
- [CrossRef] [PubMed] [Google Scholar]
- Reevaluation of the earlobe types in Koreans. Homo. 2018;69:377-80.
- [CrossRef] [PubMed] [Google Scholar]
- A study of morphological variations of the human ear for its applications in personal identification. Egypt J Forensic Sci. 2019;9:6.
- [CrossRef] [Google Scholar]
- Earlobe aging process: Elongation of the free caudal segment. Plast Reconstr Surg. 2004;113:2214-5.
- [CrossRef] [PubMed] [Google Scholar]
- A morphometric study of the external ear: Age-and sex-related differences. Plast Reconstr Surg. 2003;112:647-52. discussion 653-4
- [CrossRef] [PubMed] [Google Scholar]
- Rejuvenating earlobe esthetics with dermal fillers. J Cosmet Dermatol. 2022;21:2788-92.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsurgical treatment of earlobe aging in Mowlavi stages I and II earlobe ptosis with Hyaluronic acid fillers. J Cosmet Dermatol. 2019;18:508-10.
- [CrossRef] [PubMed] [Google Scholar]
- Ear lobule rejuvenation in face-lifting: The role of fat augmentation. Plast Reconstr Surg Glob Open. 2016;4:e597.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe rejuvenation: A fat grafting technique. Aesthet Surg J. 2016;36:872-6.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe correction of the pierced ear: A systematic review of the literature and principles for surgical reconstruction. Facial Plast Surg Aesthet Med. 2023;25:83-9.
- [CrossRef] [PubMed] [Google Scholar]
- The rolling earlobe flap for dilated ear holes following ear gauging: A novel approach to aesthetically preserving earlobe soft tissue volume. Arch Plast Surg. 2017;44:453-6.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe reduction with minimally visible scars: The sub-antitragal groove technique. Aesthetic Plast Surg. 2017;41:335-8.
- [CrossRef] [PubMed] [Google Scholar]
- Correction of pixie ear: Infraauricular skin redraping method. Arch Craniofac Surg. 2022;23:187-9.
- [CrossRef] [PubMed] [Google Scholar]
- A different approach for protruding earlobe correction-modified fish-tail technique. Aesthetic Plast Surg. 2024;48:2011-7.
- [CrossRef] [PubMed] [Google Scholar]
- Reconstruction of lost ear lobule. J Dr NTR Univ Health Sci. 2019;8:48-51.
- [CrossRef] [Google Scholar]
- Earlobe reconstruction using a Limberg flap in six ears. Br J Plast Surg. 2003;56:33-6.
- [CrossRef] [PubMed] [Google Scholar]
- Preauricular flap for post burn ear lobe reconstruction-a case report. Burns. 2000;26:571-4.
- [CrossRef] [PubMed] [Google Scholar]
- The treatment of a multisubunit defect of the earlobe involving an exposed parotid gland. Cureus. 2023;15:e50224.
- [CrossRef] [Google Scholar]
- Total earlobe reconstruction with a superiorly based preauricular flap. An Bras Dermatol. 2016;91:372-4.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe reconstruction with an inferior pedicle flap. J Plast Reconstr Aesthet Surg. 2023;80:91-3.
- [CrossRef] [PubMed] [Google Scholar]
- Freestyle perforator flap in earlobe reconstruction. BMC Surg. 2022;22:396.
- [CrossRef] [PubMed] [Google Scholar]
- Inversion of the flap at the lower ear and restoration of the flap at postauricular skin for reconstruction of the earlobe. J Craniofac Surg. 2012;23:560-2.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe reconstruction with a modified bilobed flap. Plast Reconstr Surg. 2010;126:23e-4.
- [CrossRef] [PubMed] [Google Scholar]
- Combined preauricular, retroauricular bilobed flap for earlobe reconstruction. BMJ Case Rep. 2023;16:e255982.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe reconstruction following plug and tunnel piercing. J Plast Reconstr Aesthet Surg. 2010;63:e294-5.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical correction of the expanded earlobe after ear gauging. Aesthetic Plast Surg. 2010;34:632-3.
- [CrossRef] [PubMed] [Google Scholar]
- Repair of dilated earlobe due to plug piercing. Dermatol Surg. 2010;36:1621-3.
- [CrossRef] [PubMed] [Google Scholar]
- Double opposing perpendicular linear repair of gauge ear-piercing deformity: A new technique and literature review. Eplasty. 2014;14:e31.
- [Google Scholar]
- Aesthetic earlobe reduction: A practical geometric modification with natural contour preservation. Facial Plast Surg. 2019;35:294-8.
- [CrossRef] [PubMed] [Google Scholar]
- Ear lobule rejuvenation in primary facelift. Egypt J Plast Reconstruct Surg. 2023;47:187-91.
- [CrossRef] [Google Scholar]
- Restoration of the age elongated auricular lobe. Aesthet Surg J. 2020;40:819-26.
- [CrossRef] [PubMed] [Google Scholar]
- Earlobe rejuvenation: A review of current treatment modalities. Dermatol Surg. 2023;49:253-8.
- [CrossRef] [PubMed] [Google Scholar]
- Nonablative and hybrid fractional laser skin rejuvenation. Facial Plast Surg Clin North Am. 2020;28:37-44.
- [CrossRef] [PubMed] [Google Scholar]
- Radio frequency energy for non-invasive and minimally invasive skin tightening. Clin Plast Surg. 2011;38:437-48, vi
- [CrossRef] [PubMed] [Google Scholar]
- Aesthetic earlobe remodeling: My personal experience with an LBO laser at 532 nm. J Cosmet Laser Ther. 2014;16:129-31.
- [CrossRef] [PubMed] [Google Scholar]
- Basic chemical peeling: Superficial and medium-depth peels. J Am Acad Dermatol. 2019;81:313-24.
- [CrossRef] [PubMed] [Google Scholar]
- Chemical peels. Facial Plast Surg Clin North Am. 2023;31:475-94.
- [CrossRef] [PubMed] [Google Scholar]
- Review of lasers and energy-based devices for skin rejuvenation and scar treatment with histologic correlations. Dermatol Surg. 2022;48:441-8.
- [CrossRef] [PubMed] [Google Scholar]
- Ablative laser therapy of skin. Facial Plast Surg Clin North Am. 2023;31:463-73.
- [CrossRef] [PubMed] [Google Scholar]
- A comparative study between conventional sutures, staples, and adhesive glue for clean elective surgical skin closure. Cureus. 2022;14:e31196.
- [CrossRef] [Google Scholar]
- A survey of aesthetic standards of the ear. J Craniofac Surg. 2020;31:527-9.
- [CrossRef] [PubMed] [Google Scholar]
- Split earlobe repair with piercing preservation and optimal earlobe aesthetics. J Am Acad Dermatol. 2019;80:e115-6.
- [CrossRef] [PubMed] [Google Scholar]




