
Translate this page into:
Double Triangle Suture Technique for Inverted Nipple Correction While Preserving the Lactiferous Ducts
* The two authors have contributed equally
Address for correspondence: Dr. Il Hwan Byun, Department of Plastic and Reconstructive Surgery, DA Plastic Surgery, 125 Teheran-ro, Gangnam-gu, Seoul, Korea. E-mail: byunmd@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
Inverted nipple is a relatively common symptom to encounter, and numerous surgical techniques have been developed for correction.
Aim:
The aim of this study is to provide a simple and effective procedure with long-term results.
Materials and Methods:
A total of 209 nipples of 108 patients received inverted nipple correction via double triangle suture technique.
Results:
Of the 108 patients, 7 patients had unilateral inverted nipple and 101 patients had bilateral. Of the 209 nipples operated, 28 were grade 1, 117 were grade 2, and 64 were grade 3. The mean follow-up period was 13.16 ± 6.77 months. There were minimal complications.
Conclusion:
Double triangle suture technique is a safe and reliable inverted nipple correction method. It requires two small incisions, few sutures, and minimal operation time. We especially recommend this procedure for young women with potential breastfeeding in the future and who concern for minimal scars.
Keywords
Double triangle suture
inverted nipple
lactiferous ducts

INTRODUCTION
The social demand for aesthetic procedures concerning the breast and body contour increases by year, and inverted nipple is a relatively common symptom to encounter in the clinic. Inverted nipple is defined as a flattened nipple lying on a lower plane than the areola due to shortened lactiferous ducts in fibrous bands.[12] This symptom affects up to 10% of women, often bringing distress, insecurity, and functional problems.[3456] Inverted nipple is commonly graded by the Han and Hong system, in which grade 1 nipple can be easily pulled out and maintained, grade 2 nipple can be pulled out with effort but tends to retract, and grade 3 nipple is severely retracted and very difficult to pull out manually.[7]
Several surgical techniques have been developed for inverted nipple correction, including dermoglandular flaps, endoscopic release, purse-string suturing, continuous retraction, and using artificial dermis.[58910111213] Yet, many of such procedures damage the lactiferous ducts or constrict them, possibly resulting in functional sequelae. Here, we present the methods and results of a simple, minimally invasive, and effective internal suturing technique involving two triangles.
MATERIALS and METHODS
From January 2019 to December 2020, a total of 209 nipples of 108 patients received inverted nipple correction via double triangle suture technique in our institute. We retrospectively reviewed the data on demographics, surgical procedure, and complications. The study was performed in accordance with the Declaration of Helsinki.
Thorough history taking was done preoperatively including comorbidities, medications, allergies, surgical history, drinking, and smoking history. Drinking and smoking cessation was strongly recommended before and after the surgery.
All operations were performed under local anesthesia, unless the procedure was combined with other breast surgeries such as augmentation mammoplasty under general anesthesia. Local anesthetic of 1% lidocaine mixed with 1:100,000 epinephrine solution was injected along the base of the nipples, near 3, 6, 9, and 12 o’clock directions. Traction sutures were done with nylon 5-0 on the top of both nipples. Gently pulling the traction suture, two small slit incisions (2 mm) were made with surgical blade at the base of 3 and 9 o’clock positions. Through the small incisions, resistant collagen fibers were thoroughly and circumferentially released with curved Metzenbaum scissors. This releasing process is vital for successful correction, and the curved scissors should not intrude the center of the nipple for the preservation of the lactiferous ducts. After thorough release of the nipple, the first triangle suture was done starting from the 3 o’clock incision with nylon 5-0. This suture exits and re-enters the nipple from 12 o’clock direction, passing through the 9 o’clock incision, and then back to the original 3 o’clock incision. This creates a slightly curved triangle, and the triangle also should not intrude the core of the nipple. The suture was tied, and the knot was buried in the starting incision. Then the second triangle suture was created in the same manner, except starting from the opposite 9 o’clock incision to 6 o’clock direction. After two triangle sutures were done, the two slit incisions were sutured with nylon 6-0. Schematic drawing of the procedure is shown in Figure 1. After the surgery, the patients were advised not to wear compressive brassieres for at least 2 weeks.
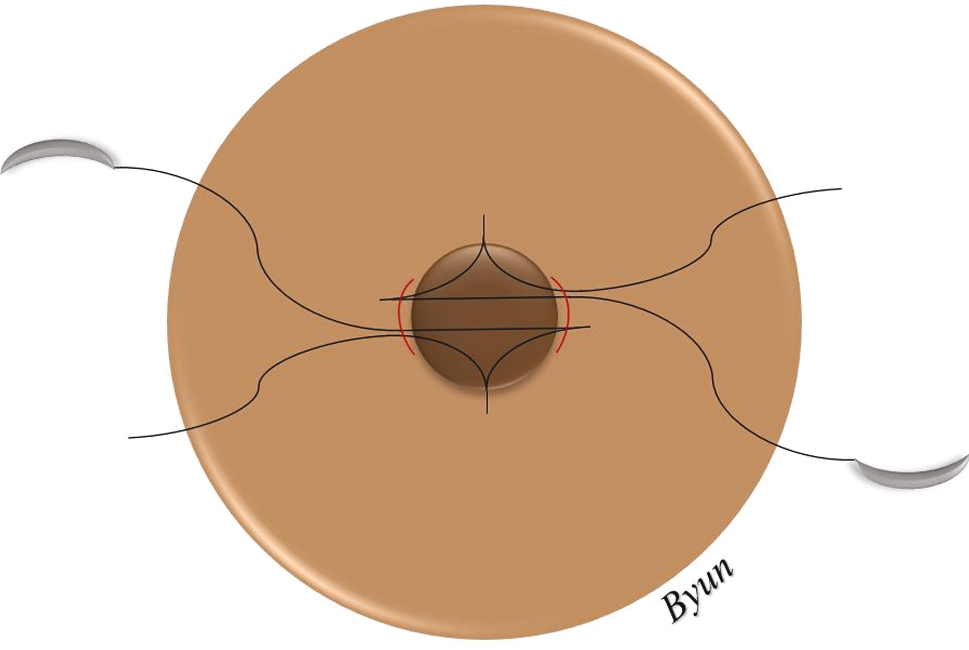
- Schematic drawing of the double triangle suture technique for inverted nipple correction
RESULTS
Of the 108 patients included in this study, all of them were females with the mean age of 27.39 ± 6.74 and mean body mass index of 22.28 ± 4.13. Seven patients had unilateral inverted nipple and 101 patients had bilateral. Of the 209 nipples operated, 28 were grade 1, 117 were grade 2, and 64 were grade 3. The mean follow-up period was 13.16 ± 6.77 months. Other demographic data and surgical details are listed in Table 1.
| Number of patients | 108 (209 nipples) |
| Unilateral | 7 (6.48%) |
| Bilateral | 101 (93.52%) |
| Age (years) | 27.39 ± 6.74 |
| Sex | |
| Male | 0 (0%) |
| Female | 108 (100%) |
| Grade | |
| 1 | 28 (13.40%) |
| 2 | 117 (55.98%) |
| 3 | 64 (30.62%) |
| Body mass index (BMI) | 22.28 ± 4.13 |
| Comorbidities | |
| Hypertension | 1 (0.93%) |
| Diabetes | 0 (0%) |
| Smoking | 5 (4.63%) |
| Follow-up period (months) | 13.16 ± 6.77 |
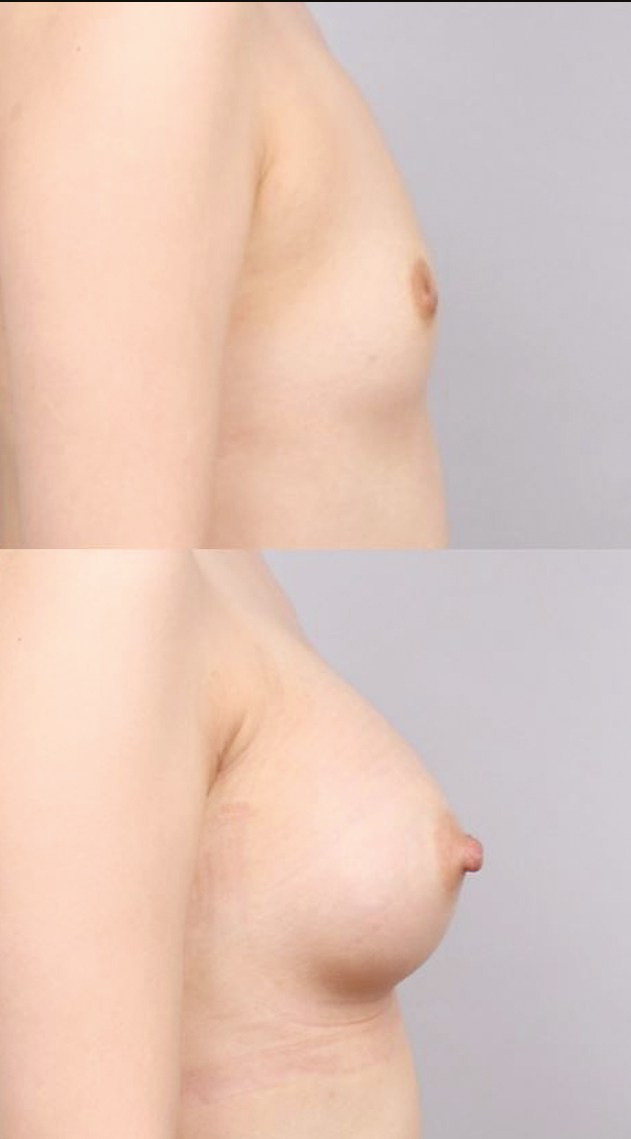
There were few complications following our operation. One nipple (0.48%) showed wound dehiscence and was re-sutured in the outpatient clinic without further sequelae. Three nipples (1.44%) showed partial recurrence, and re-operations were done with the same double triangle suture technique. All patients including those who underwent re-operation showed satisfactory final results and no sensory loss or necrosis. Further details are listed in Table 2. The pre- and postoperative photographs of some of our patients are shown in Figures 2 and 3.
| Hematoma | 0 (0%) |
| Infection | 0 (0%) |
| Wound dehiscence | 1 (0.48%) |
| Nipple necrosis | 0 (0%) |
| Hypertrophic scar | 0 (0%) |
| Permanent sensory loss | 0 (0%) |
| Partial recurrence | 3 (1.44%) |

- Preoperative (above) and postoperative (below) 1-year views of a 29-year-old female who received inverted nipple correction
- Preoperative (above) and postoperative (below) 1-year views of a 24-year-old female who received inverted nipple correction with augmentation mammoplasty
DISCUSSION
The demand of inverted nipple correction closely follows the increasing trend of breast augmentation. Augmentation mammoplasty is the most common cosmetic surgery in the USA and is growing very popular in Asia as well.[14] More and more young women receive breast augmentation, and those who have inverted nipples often want them corrected as well. Because of the young age of many patients, preserving the lactiferous ducts is important for future potential breastfeeding. Yet many of the traditional techniques for inverted nipple correction involve dermal flaps and turnover flaps, giving injury to the mammary ducts.[812,151617] Concerning future duct functions as well as postoperative scars, less invasive techniques are more favorable for young women. Some surgeons presented several internal suture and purse-string techniques; yet those methods inherently increase tension on the central portion of the nipple, possibly interfering with the ducts function.[410,181920]
Our technique manipulates two internal triangle sutures on the superior and inferior portions of the nipple and has several strengths. Besides the time efficiency and minimal invasiveness, our technique does not bring tension to the center of the nipple. When the two triangle sutures are tied, they pull the upper and lower portions of the nipple separately, expanding the central portion. This effectively preserves the central lactiferous ducts. Although there are chances of cheese-wiring, as with other purse-string techniques, the separate sutures may provide better stability and longevity. Also, in comparison to several previous studies which used absorbable 3-0 or 4-0 sutures, we used non-absorbable nylon 5-0 sutures.[419] Although there is no single answer, we believe that thin 5-0 sutures are less painful and sufficient for this procedure and non-absorbable sutures provide better longevity. We did not have any infection complications.
Our study and technique are not without limitations. Our mean follow-up period was 13.16 ± 6.77 months, and greater follow-up period and sample size will strengthen our results. Also, as mentioned earlier, many young women received combination operations of breast augmentation and inverted nipple correction. The two procedures are synergistic, and augmentation itself alleviates the inverted nipple symptom. We especially recommended combinative surgery for those with grade 3 inverted nipple, and thus one may think that the results are partly masked. Yet, nearly half of grade 3 patients received inverted nipple correction alone and yielded satisfactory results.
CONCLUSION
Here, we described a safe and reliable inverted nipple correction technique involving double triangle sutures. It requires two small incisions, few sutures, and minimal operation time. We especially recommend this procedure for young women with potential breastfeeding in the future and who concern for minimal scars.
Financial support and sponsorship
None.
Conflicts of interest
The authors declare that there are no conflicts of interest.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
REFERENCES
- Alternative nipple suspension technique in the treatment of inverted nipple: Reverse s-shaped design. J Cutan Aesthet Surg. 2014;7:220-3.
- [Google Scholar]
- Correction of inverted nipple: An alternative method using two triangular areolar dermal flaps. Ann Plast Surg. 2003;51:636-40.
- [Google Scholar]
- Inverted nipple repair revisited: A 7-year experience. Aesthet Surg J. 2015;35:156-64.
- [Google Scholar]
- Correction of inverted nipples by strong suspension with areola-based dermal flaps. Plast Reconstr Surg. 2007;120:1483-6.
- [Google Scholar]
- Correction of the severely inverted nipple: Areola-based dermoglandular rhomboid advancement. J Plast Reconstr Aesthet Surg. 2011;64:e297-e302.
- [Google Scholar]
- The inverted nipple: Its grading and surgical correction. Plast Reconstr Surg. 1999;104:389-95; discussion 396-7.
- [Google Scholar]
- Simple technique for correction of inverted nipple. Plast Reconstr Surg. 1980;65:504-6.
- [Google Scholar]
- The endoscope as an adjunct to correction of nipple inversion deformity. Plast Reconstr Surg. 2007;119:1178-82.
- [Google Scholar]
- Correction of the inverted nipple with an internal 5-point star suture. Ann Plast Surg. 2004;53:293-6.
- [Google Scholar]
- Correction of inverted nipple: An alternative method using continuous elastic outside distraction. Ann Plast Surg. 2005;54:120-3.
- [Google Scholar]
- Correction of inverted nipple using strut reinforcement with deepithelialized triangular flaps. Plast Reconstr Surg. 1998;102:1253-8.
- [Google Scholar]
- A method for correcting an inverted nipple with an artificial dermis. Aesthetic Plast Surg. 2004;28:233-8.
- [Google Scholar]
- Current trends in breast augmentation: An international analysis. Aesthet Surg J. 2018;38:133-48.
- [Google Scholar]
- Pursestring technique for treatment of nulliparous congenital inverted nipple. J Cutan Aesthet Surg. 2021;14:84-7.
- [Google Scholar]
- The application of de-epithelialised “turn-over” flaps to the treatment of inverted nipples. Br J Plast Surg. 1984;37:253-5.
- [Google Scholar]
- Inverted nipple correction using a combination of the perpendicular suture method and the purse-string suture method. Arch Aesthetic Plast Surg. 2017;23:104-7.
- [Google Scholar]
- Inverted nipple treatment and poliglecaprone spacer. Aesthetic Plast Surg. 2018;42:958-63.
- [Google Scholar]
- Minimally invasive correction of inverted nipples: A safe and simple technique for reliable, sustainable projection. Ann Plast Surg. 2009;62:549-53.
- [Google Scholar]




