
Translate this page into:
In vivo dermabrasion for de-epithelialization of autologous composite fat and dermal micrograft for treatment of small localized depressed scars
*Corresponding author: Somesh Gupta, Department of Dermatology and Venereology, All India Institute of Medical Sciences, New Delhi, India. someshgupta@aiims.edu
-
Received: ,
Accepted: ,
How to cite this article: Taneja N, Gupta S. In vivo dermabrasion for de-epithelialization of autologous composite fat and dermal micrograft for treatment of small localized depressed scars. J Cutan Aesthet Surg. doi: 10.25259/jcas_12_24
Dear Editor,
The available therapeutic options for the correction of volume loss in localized depressed scars include synthetic fillers, autologous fat, and cultured fibroblasts. Their use is limited by the temporary effect, foreign body reaction, and/or high cost.1 De-epithelialized macrografts and micrografts have been used to fill these defects.1 The de-epithelialization is done using a sharp dissection after obtaining the graft, which is technically challenging, less precise, and often leads to loss of the dermal tissue.2
We propose harvesting composite dermal and fat micrografts from the dermabraded donor site, creating a micrograft suspension, and filling small localized depressed scars. The procedure is carried out under topical anesthesia with eutectic mixture of local anesthetics (EMLA®) (lignocaine + prilocaine) on the recipient site and infiltration anesthesia at the donor site (upper thigh). The donor epidermis is removed using a motorized dermabrader fitted with a diamond burr. Then, multiple punch biopsies (1.5 mm–2 mm) are obtained [Figure 1a and b]. Deep biopsies containing both dermis and subcutaneous fat are collected in a sterile petri dish and minced mechanically using a surgical blade to make a uniform suspension [Figure 1c]. There is no storage or conditioning media required during the mincing and preparation of suspension. The suspension is transferred to a 1 mL syringe which is then injected into the defect through an 18G needle after doing subcision with the same needle [Figure 1d]. Due to the subsequent decrease in graft size after implantation over a few months, overcorrection of up to 20–30% is recommended to overcome the loss in filling volume. Then, the entry point of the needle on the recipient area is sealed with a Steri-Strip.
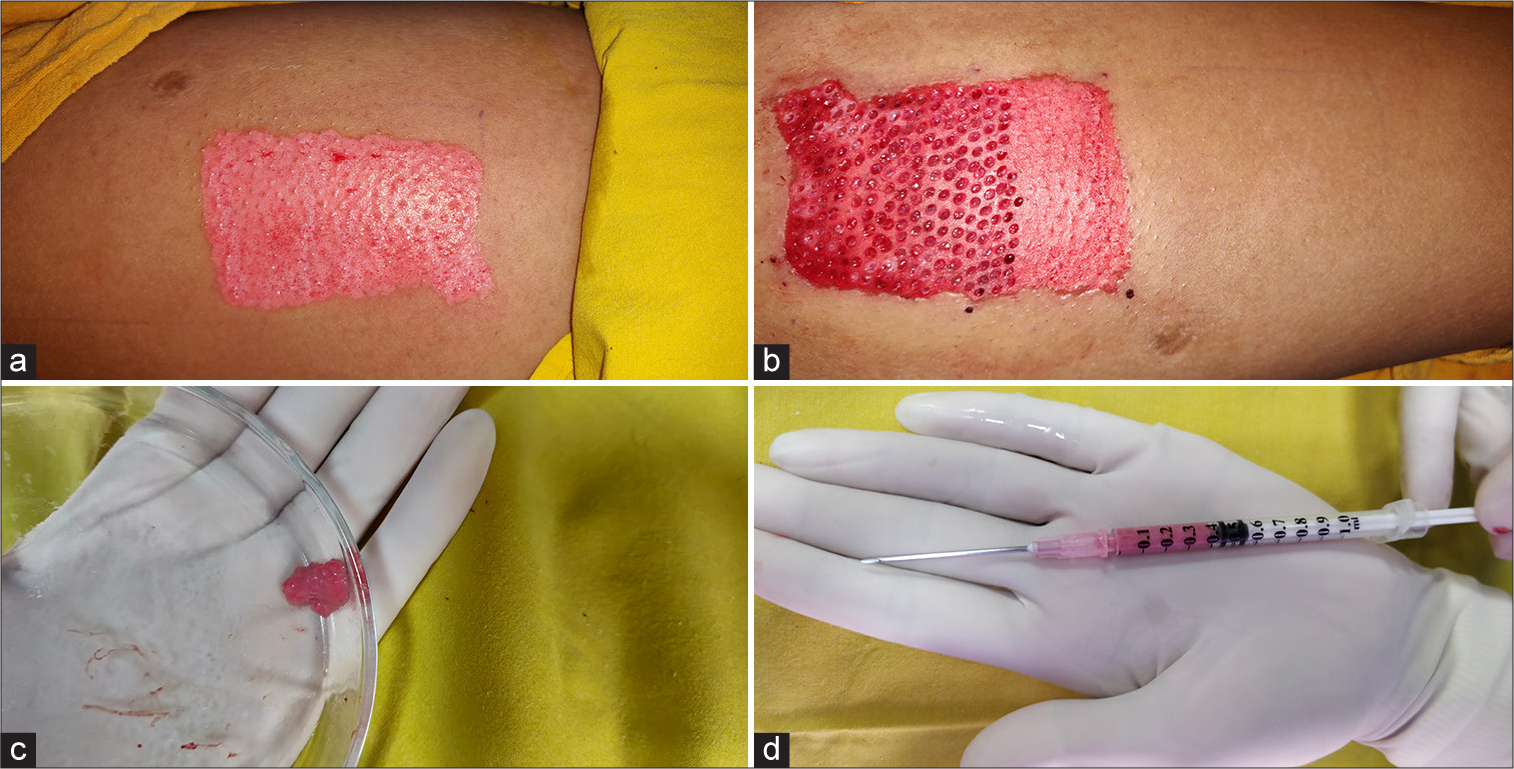
- (a) De-epithelized area done with motorized dermabrader; (b) multiple closely-spaced 1.5 mm punch biopsies taken from de-epithelized area; (c) the biopsies containing dermis and fat are minced and prepared into a suspension in a petri dish; and (d) the suspension is transferred into 1 ml syringe attached to an 18 G needle, for injecting.
The patients have significant elevation in the depressed scars, and the facial volume loss is restored [Figure 2]. The donor site healed well in 1 week, with minimal scarring.
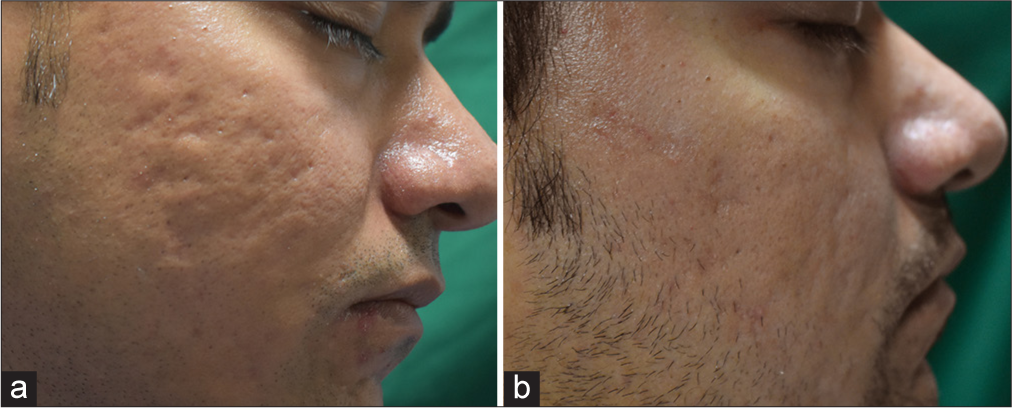
- (a) Depressed acne scars; and (b) results after 3 months of injecting autologous composite fat and dermal micrograft.
The procedure of harvesting, preparing, and injecting the micrograft is easy, inexpensive, and effective for small, depressed scars.
Authors’ contributions
Both the authors were involved in concepts, design, definition of intellectual content, literature search, data acquisition, manuscript preparation, manuscript editing and manuscript review.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Autologous smashed dermal graft with epidermal re-closure: Modified technique for acne scars. J Cutan Aesthet Surg. 2016;9:258-62.
- [CrossRef] [PubMed] [Google Scholar]
- Deepithelialized flaps and grafts: Applications in dermatologic surgery. Cutis. 2018;101:213-6.
- [Google Scholar]




