
Translate this page into:
Innovative technique for partial earlobe tear repair using a customized elliptical biopsy punch
*Corresponding author: Akshay Arun Vetal, Department of Dermatology, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, Maharashtra, India. akkiii5858@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vetal AA, Dhurat RS, Chethan MV, Jain D. Innovative technique for partial earlobe tear repair using a customized elliptical biopsy punch. J Cutan Aesthet Surg. doi: 10.25259/JCAS_49_2024
Abstract
Incomplete split earlobes, frequently resulting from heavy and pendulous ear jewelry, can cause significant cosmetic and psychological distress. Traditional lobuloplasty techniques often face challenges, particularly in achieving precise and symmetrical results. This study introduces an innovative lobuloplasty technique using a customized elliptical biopsy punch to repair Type I and Type IIA earlobe deformities. By modifying a standard circular biopsy punch, we achieved better margin symmetry and tissue approximation. The procedure involves a two-stage process of stamping and circumduction to excise the defect, followed by closure with vertical mattress sutures. This technique offers several intraoperative advantages, including reduced tissue handling, minimized blood loss, and time efficiency, leading to superior cosmetic outcomes. Our findings suggest that this method is a significant improvement over conventional techniques, providing a more user-friendly approach and enhanced patient satisfaction.
Keywords
Elliptical biopsy punch
Types of earlobe tear
Lobuloplasty
Time saving
Better cosmetic outcomes

PROBLEM STATEMENT
Earlobe piercing is a common practice worldwide. In the Indian subcontinent, it has deep cultural roots. It is also used as a fashion statement and a form of self-expression in modern times. A common complication of earlobe piercing is the eventual widening of the ear hole. Common causes include the usage of heavy and pendulous ear jewelry. Chronic traction on the earlobe by the jewelry results in atrophy of tissue and gradual widening of the ear hole, subsequently leading to a split earlobe.1 This problem often compels patients to avoid wearing small ear studs as they may not fit well and fall off.
Sadasivan and Kochunarayan proposed a revised classification of split earlobe deformity in 20202 [Figure 1]:

- Types of Earlobe tear: (a) Type I: Elongated perforation with length less than that of normal tissue, (b) Type IIA: Elongated perforation with length more than that of normal tissue measured from the lower end of the cleft to the inferior margin of the earlobe, (c) Type IIB: Inferior contour abnormal, and (d) Type III- Total earlobe tear.
Type I: Elongated perforation with a length less than that of normal tissue
Type IIA: Elongated perforation with length more than that of normal tissue measured from the lower end of the cleft to the inferior margin of the earlobe
Type IIB: Inferior contour abnormal, ptosis of earlobe present
Type III: Total earlobe tear.
The earlobe is one of the most fleshy and mobile areas on the body, making it difficult to keep steady during cosmetic repair. Maintaining linear cuts is challenging, especially with the earlobe’s tendency to slip during handling. For Type I and Type IIA earlobe tear repair, traditional methods often involve freshening the cleft margins by excising cleft tissue with a scalpel.3 However, incomplete excision or over-excision can result in grooving along the suture line, notching of the inferior margin, and contour irregularities. Creating equal margins on both sides of the cleft is challenging. In addition, this method is time-consuming, as incisions are required over the lateral as well as the medial aspect of the earlobe. Maintaining hemostasis is another challenge due to the time-consuming nature of the procedure.
RECOMMENDED SOLUTION
In this modified technique, we converted a traditional circular 5 mm biopsy punch into an elliptical one [Figure 2]. The biopsy punch was compressed on both ends using artery forceps to create an elliptical cutting edge with two symmetrical arcs that intersected at an angle of 30° or less [Video 1]. Depending on the length of the Type I and Type IIA earlobe, a punch of a smaller or larger size was used. The earlobe was held in place using a chalazion clamp. The flat surface was placed against the medial aspect of the earlobe, and the ring was placed over the lateral aspect such that the ear hole lay in the center. The clamp was then tightened.
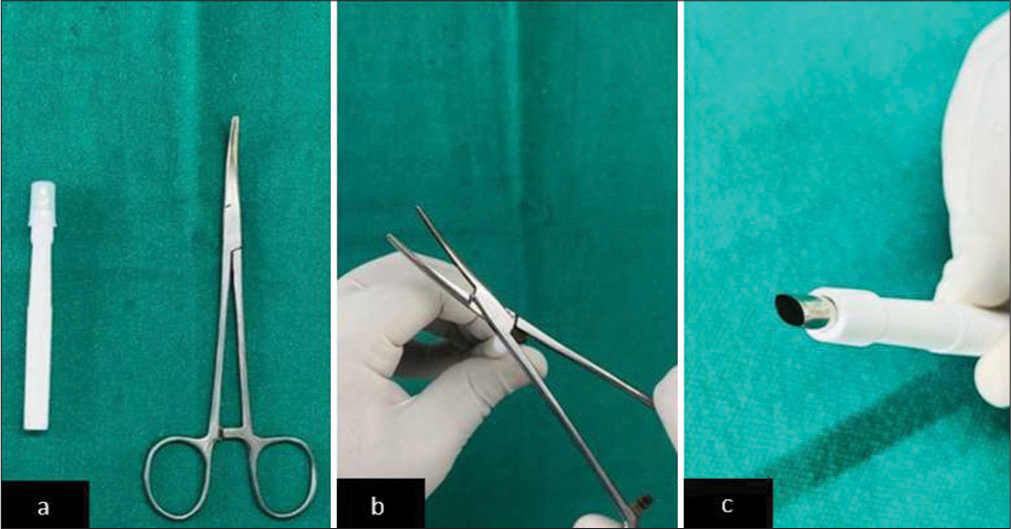
- (a) Biopsy punch and artery forceps, (b) compressing the biopsy punch to give elliptical margins, and (c) biopsy punch with uniform margin and angle of 30° at each margin.
Video 1:
Video 1:Process of modifying the biopsy punch.The innovative technique involved two main stages: Stamping and circumduction movement [Video 2]. The initial step involved positioning the oval punch over the enlarged ear hole and applying firm, even pressure, to create an imprint. This “stamp” marked the boundaries of the area to be excised, providing a guide for the next step. Following the initial imprint, the punch was carefully rotated by a circumduction movement while maintaining pressure. The punched-out area was then excised, similar to a skin biopsy sample, providing a cylindrical tissue sample with skin at both ends. The defect on the earlobe was closed with non-absorbable polypropylene intermittent vertical mattress sutures on the lateral as well as medial aspects [Figure 3].
Video 2:
Video 2:Stamping and circumduction movement.
- (a) Pre-operative photo showing Type I deformity, (b) intraoperative photo showing a through and through a slit in the earlobe after punching, (c) post-operative photo after closing the slit with vertical mattress sutures, and (d) post-operative picture on day 10.
This technique provides several advantages over the conventional method:
The punch design ensures equal margin lengths on both sides, better approximation, and better cosmetic outcomes
-
Reduced tissue handling and damage, as there is no need to excise tissue from both the medial and lateral sides of the lobule [Figure 4]
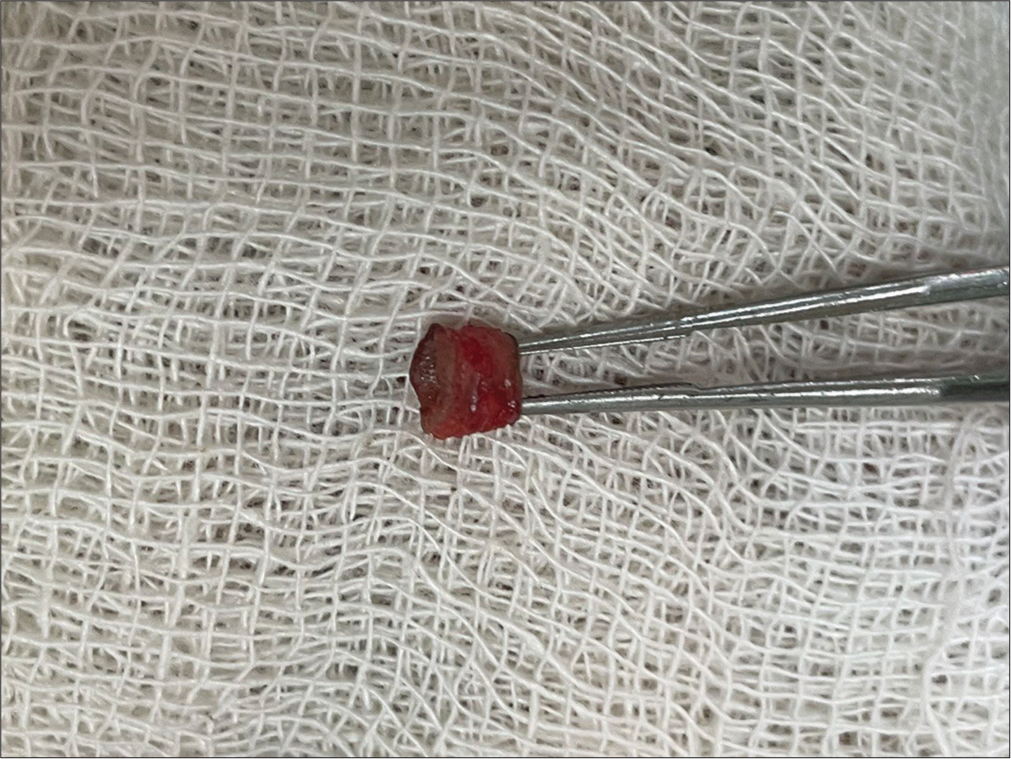 Figure 4:
Figure 4:- Cylindrical tissue sample with the skin at both ends and the cleft at its center along its length.
Reduced blood loss
Time-saving
Smooth contour of the earlobe post-procedure.
The use of an oval biopsy punch for lobuloplasty provides several advantages over the conventional technique. It has a friendlier learning curve, is less time-consuming, and results in satisfactory cosmetic outcomes.
Authors’ contributions
Dr Akshay Vetal: Concept, design, definition of intellectual content, data analysis, literature research, manuscript preparation statistical analysis, manuscript editing and review, literature search. Dr Rachita Dhurat: Clinical studies, data analysis, statistical analysis, literature research, manuscript editing and review. Dr Chethan MV: Data acquisition, literature research. Dr Darshan Jain: Literature research, manuscript preparation.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Videos available on:
Financial support and sponsorship
Nil.
References
- Repair of a split or deformed ear lobe with a tongue depressor blade for stabilization during surgery In: Innovative techniques in skin surgery Vol 9. (1st ed). United States: CRC Press; 2002. p. :531-4.
- [CrossRef] [Google Scholar]
- A revised classification and treatment algorithm for acquired split earlobe, with a description of the composite technique and its outcome. Cureus. 2020;12(6):e10422.
- [CrossRef] [PubMed] [Google Scholar]
- The cleft earlobe: A review of methods of treatment. Ann Plast Surg. 1994;33:677-80.
- [CrossRef] [PubMed] [Google Scholar]




