
Translate this page into:
Platelet rich fibrin membrane: An effective biological dressing for the regeneration of lip defects – A case report

*Corresponding author: Deepak Singh, Department of Oral and Maxillofacial Surgery, Rural Dental College, Pravara Institute of Medical Sciences, Loni, Maharashtra, India. dsomfs2@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Singh D, Sansgiri TS, Saluja H, Shah SV. Platelet rich fibrin membrane: An effective biological dressing for the regeneration of lip defects – A case report. J Cutan Aesthet Surg. doi: 10.25259/jcas_39_23
Abstract
The face is a highly esthetic zone. Any facial injuries if not treated in tiSme can cause disfigurement and have a detrimental effect on the quality of life of the individual. Many studies are done in the field of tissue engineering which involves the application of growth factors to regenerate the lost facial tissues for a better esthetic outcome. Platelet concentrates (PCs) are widely used in the medical field for the regeneration of soft tissue. Platelet-rich fibrin (PRF) is a second-generation PC that consists of a fibrin matrix polymerized in a tetra molecular structure that incorporates platelets, leucocytes, cytokines, and circulating stem cells. PRF membrane can be used as a biological dressing over maxillofacial wounds. This case report presents a unique way of regenerating the lost soft tissue of the lip by local application of PRF membranes as a biological dressing.
Keywords
Biological dressing
Platelet-rich fibrin
Lower lip defect

INTRODUCTION
Injuries to the soft tissue of the face can cause disfigurement and have a detrimental effect on the quality of life of the individual. Therefore, managing the soft-tissue defects of the face becomes a challenging task for an oral and maxillofacial surgeon because the main aim of the treatment is to restore function as well as esthetics. Wound healing is a complex process that involves a cascade of intracellular and extracellular events. Over the past decade, there has been a lot of advancement in the field of tissue engineering which involves the application of growth factors that will regenerate, enhance, or replace the damaged or missing tissues.1,2
Tremendous research has been done on platelet concentrates (PCs), which are widely used in the medical field for the regeneration of soft tissues. Platelet-rich fibrin (PRF) is a second-generation PC that consists of a fibrin matrix polymerized in a tetra molecular structure that incorporates platelets, leucocytes, cytokines, and circulating stem cells.3 This case report presents a unique way of regenerating the lost soft tissue of the lip by local application of PRF as a biological dressing.
CASE REPORT
A 19-year-old boy reported to the Department of Oral and Maxillofacial Surgery with a history of road traffic accident while riding a two-wheeler, following which he sustained an avulsive soft-tissue defect on the left corner of the upper lip. The lip defect measured approximately 1.5 × 1.0 × 0.5 cm with disruption of the vermilion border and white roll [Figure 1]. The depth of the defect involved the entire thickness of the lip with partial loss of muscle tissue. The patient was not willing to reconstruct the defect with local flaps. Since the patient was young, it was decided to reconstruct the lip defect using PRF dressings.

- Avulsive soft-tissue defect on the left corner of the upper lip measuring approximately 1.5 × 1.0 × 0.5 cm with disruption of the vermilion border and white roll.
Method of preparing PRF membrane
Around 5 mL of whole venous blood was collected in each of the two sterile vacutainer tubes of 6 mL capacity without anticoagulant. The vacutainer tubes were then placed in a centrifugal machine at 3000 revolutions per minute (rpm) for 10 min. The fibrin clot obtained from the middle part of the tube was then flattened to form the PRF membrane [Figure 2].
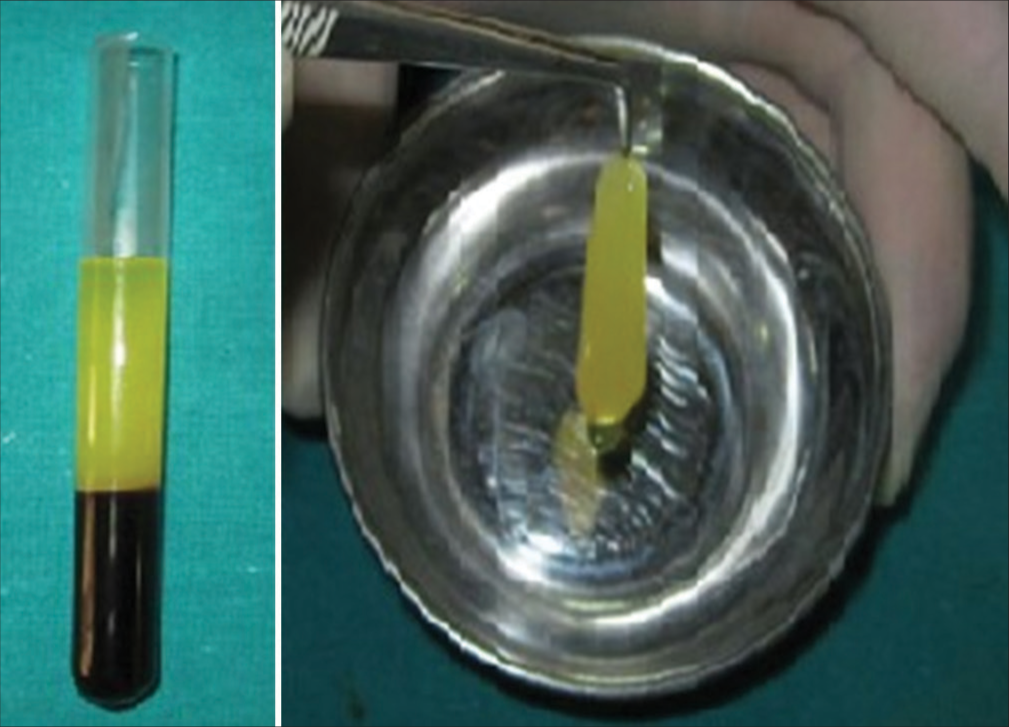
- Preparation of platelet-rich fibrin.
The PRF membrane was sutured to the margins of the defect using 4–0 prolene [Figure 3]. The patient was recalled after 1 week, suture removal was done, the margins were revised, and a new PRF membrane dressing was done over the defect [Figure 4]. A total of five PRF membrane dressings were given. In the subsequent visits, a gradual decrease in the size of the defect was seen with no signs of inflammation and infection [Figure 5]. The regenerated lip tissue was comparable with the adjacent uninjured tissue. The defect in the vermillion and the white role was inconspicuous [Figures 6 and 7]. At the end of 3 months, complete regeneration of the lip tissue was seen.

- Platelet-rich fibrin membrane sutured to the lip defect with 4–0 prolene.

- 3rd follow-up visit.

- Gradual decrease in the size of the defect (red arrow) with no signs of inflammation and infection.

- Satisfactory regeneration of the lost lip tissues at the end of 3 months.

- The defect in the vermillion and the white role is inconspicuous.
DISCUSSION
Managing maxillofacial injuries is challenging for an oral and maxillofacial surgeon, as the face is a highly esthetic area. Wound healing is a complex cascade of intracellular and extracellular events that are regulated by signaling proteins.4
One of the most undesirable complications of wound healing is the formation of a scar. This can be minimized by primary closure, but in cases where the defect is large, it becomes difficult to achieve primary closure. In such cases, the reconstruction can be done with local/regional flaps or microvascular flaps.
There has been a lot of research in the field of tissue engineering. Newer materials and techniques have been introduced to improve the outcomes of wound healing. Apart from hemostasis, studies show that platelets play a crucial role in wound healing and tissue regeneration, because they release growth factors, cytokines, and extracellular matrix modulators that help in angiogenesis, restoration of damaged connective tissue, and promote proliferation and differentiation of mesenchymal stem cells into tissue-specific cell types.5,6
Over the years, PCs have gained a lot of popularity. PCs are biological autologous products that are derived from the patient’s whole blood. It consists of supraphysiological concentrates of platelets and growth factors. PCs are of two types: Platelet-rich plasma (PRP) and PRF which can be pure (i.e., P-PRP and P-PRF) or rich in leukocytes (i.e., L-PRP and L-PRF).7
PRF is a second-generation PC. It can be prepared using a simple and inexpensive method without the addition of anticoagulant at 3000 rpm for 10 min. This increases the platelet count by 1–2 folds.7,8 The slow polymerization generates a fibrin network that enhances cell migration and proliferation. It also acts as a reservoir of platelets, leukocytes, and growth factors.9 PRF can be used as a gel form which can be directly applied on the surgical site or in the form of membrane to cover bone grafts in ridge augmentation procedures.10
In the present case, primary closure was not possible and healing by secondary intention could have resulted in fibrosis and development of a hideous scar. Therefore, it was decided to treat the defect with local application of PRF membrane. PRF membranes were used as biological dressings to fill and cover the lip defects [Figures 3 and 4]. Such PRF dressings were placed at every follow-up visit. The PRF membrane protects the open wound, favors microvascularization, and accelerates healing. PRF releases an array of growth factors such as platelet-derived growth factor (PDGF)-AA, PDGF-AB, PDGF-BB, transforming growth factor-beta (TGF-Beta), vascular endothelial growth factor (VEGF), and Insulin like growth factor (IGF) to the surrounding microenvironment which contributes to the development of the three important factors of healing and soft-tissue maturation, namely, angiogenesis, immunity, and epithelial cover.1
In the subsequent follow-up visits, a gradual decrease in the size of the wound was seen [Figure 5]. The PRF-treated site showed hastened healing with early wound contracture [Figures 6 and 7]. In the present case report, the patient was satisfied with the results; therefore, no further treatment was given.
Similar results were seen by Eshghpour et al. in their case report of a 24-year-old male who was treated with PRF membranes for periorbital skin defect.10 Dohan et al (2006) found that autologous platelet gel used on skin wounds, not only enhanced wound closure but also increased the wound healing velocity.8
Desai et al. termed this type of wound healing as “modified secondary intention healing.”1 The success of this type of treatment depends on the local delivery of an array of growth factors and proteins in a fibrin network. Finally, it results in scarless esthetic wound healing. However, patient compliance also plays a crucial role.
CONCLUSION
PRF is a safe and cost-effective biological dressing for managing maxillofacial defects with excellent esthetic outcomes and a shorter recovery period, thereby improving the patient’s quality of life.
Author’s contribution
All the authors contributed to the research study. Deepak Singh: conceptualization, investigation, original draft preparation. Tanvy S. Sansgiri: conceptualization, investigation, original draft preparation, writing. Harish Saluja & Seemit V. Shah validation, review, editing.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Use of platelet-rich fibrin over skin wounds: Modified secondary intention healing. J Cutan Aesthet Surg. 2013;6:35-7.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin and soft tissue wound healing: A systematic review. Tissue Eng Part B Rev. 2017;23:83-99.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-Rich fibrin: A second generation platelet concentrate and a new friend of oral and maxillofacial surgeons. Ann Maxillofac Surg. 2011;1:53-7.
- [CrossRef] [PubMed] [Google Scholar]
- Platelets in wound healing: What happens in space? Front Bioeng Biotechnol. 2021;9:716184.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet lysates promote mesenchymal stem cell expansion: A safety substitute for animal serum in cell-based therapy applications. J Cell Physiol. 2005;205:228-36.
- [CrossRef] [PubMed] [Google Scholar]
- Regenerative effect of platelet concentrates in oral and craniofacial regeneration. Front Cardiovasc Med. 2019;6:126.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part II: Platelet-related biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2006;101:e45-50.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2006;101:e37-44.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-rich fibrin: An autologous fibrin matrix in surgical procedures: A case report and review of literature. Iran J Otorhinolaryngol. 2012;24:197-202.
- [Google Scholar]




