
Translate this page into:
Scalp Defect Reconstruction with Triple Rotation Flap: A Case Report
Address for correspondence: Dr. Kanathur Shilpa, Assistant Professor, Department of Dermatology, BMCRI, Bengaluru - 560 002, Karnataka, India. E-mail: shilpakvinod@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Scalp surgeries are some of the surgeries frequently performed in dermatosurgery department. These surgical procedures may leave large defects, especially when performed for malignant condition in which wide margin has to be excised. Such large defects are difficult to close primarily when reconstruction with local flap is essential. Here we report a case of epithelioid angiosarcoma of the scalp in a 24-year-old man where excision and reconstruction were performed using triple rotation flap.
Keywords
Reconstruction
scalp defects
triple rotation

INTRODUCTION
Scalp lesions remain a challenge for reconstructive surgery because of the poor skin mobility of the region that, among other reasons, hinders the suturing of moderate- and large-sized injuries.[1] Scalp defects following excision of skin tumors can be closed with many approaches depending on their location, size, and depth.[2] Small-to-moderate defects can be reconstructed using local flaps. The correct design of such flaps includes preservation of the original hairline, acceptable redirectioning of the hair follicles, incorporation of large vascular pedicles, and wound closure without excessive tension.[2]
Rotation flaps constitute a time-honored method for repair of small-to-moderate scalp defects, in effect even in the era of microsurgical reconstruction.[3] Here we report a case of reconstruction of moderate-sized defect of the scalp using triple rotation flap.
CASE REPORT
A 24-year-old male patient presented to dermatology department with a history of rapidly growing skin lesion over the scalp. The lesion started around 3 months back and rapidly increased to the present size of 5-cm diameter. Lesion was asymptomatic and was associated with loss of hair over the lesion. Punch biopsy of the lesion showed features suggestive of Kaposi’s sarcoma with advice for excision biopsy.
After ruling out retropositive status and relevant investigations, case was posted for excision. Scalp being the vascular structure, surgery was planned under tumescent anesthesia. Lesion was excised with inclusion of 1-cm margin of clinically normal tissue [Figure 1]. After excision, a circular defect of around 7-cm diameter was formed. Around the primary defect, three flaps were raised by marking an arc around the defect, length of the arc being 1.5 times the diameter of the defect and the angle of the arc was 30°–50° [Figure 2]. With good undermining, the three arcs were rotated into the defect and sutured at the center subdermally with Vicryl 3-0 (Ethicon, Somerville, New Jersey) [Figure 3]. The three secondary defects were closed using Prolene 3-0 (Ethicon, Somerville, New Jersey) so that the suture line resembled a fan-shaped pattern [Figure 4]. Dog ear formed at the edges was corrected using two-flap technique. A pressure dressing was put. Postoperative period was uneventful.
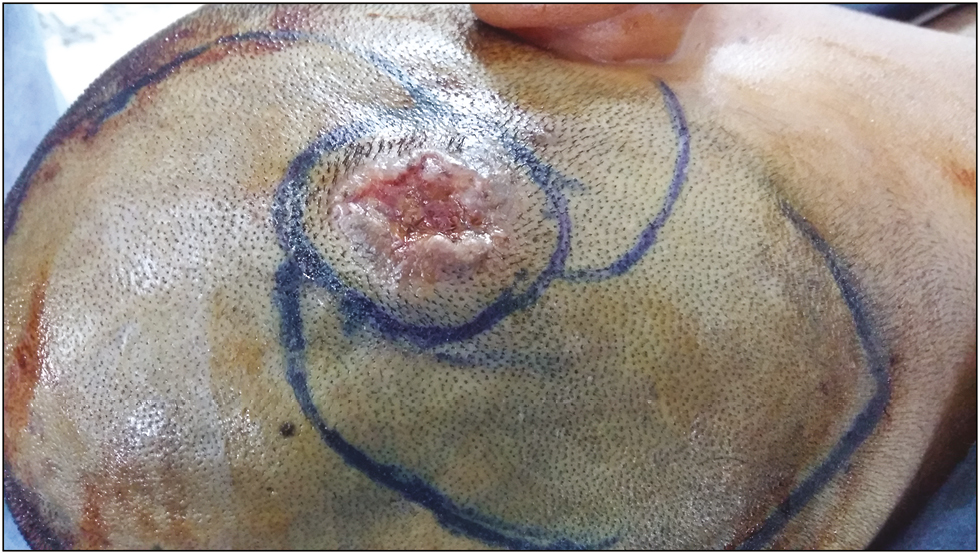
- Triple rotation planned with wide excision of tumor
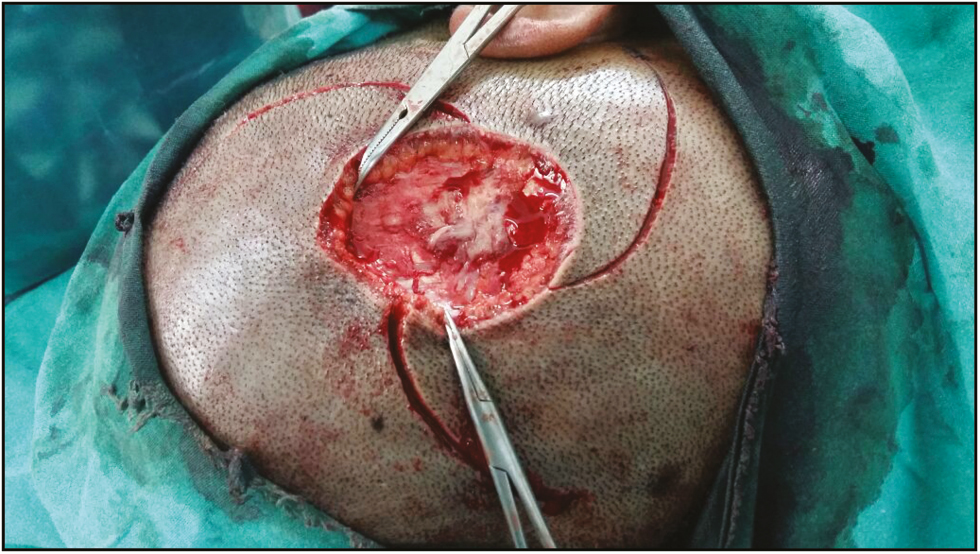
- Primary defect formed after excision along with three flaps being raised around the defect

- Three flaps rotated into the defect with three secondary defects formed

- Three flaps being closed in a fan-shaped pattern
Histopathological examination and immunohistochemistry studies of the excised specimen confirmed the diagnosis of epithelioid angiosarcoma. The margin of the specimen was free of tumor cells. However, in view of high recurrence and mortality associated with the condition, patient was further subjected to radiotherapy. Patient is under follow-up for 6 months without any recurrence.
DISCUSSION
The closure of primary defect following excision of extensive malignant neoplasms of the scalp remains a challenge for dermatosurgeons. There are various options available in the management of scalp defects, which include full-thickness grafts, local flaps, pedicle grafts, and tissue expanders. The choice of procedure depends on the predisposing condition, site of the defect, size of the defect, direction of hair, and functional and aesthetic outcome. Because of the anatomy of the scalp and its high vascularity, with anastomoses between the main vascular pedicles, different types of flaps may be used with satisfactory results. The most commonly used are the random flap, which does not have a defined pedicle, and the axial flap, which is used in situations in which a defined vascular pedicle is present.[3] The rotation flap is among the most commonly used local flaps for this region; this involves the rotation of a semicircular segment of skin, subcutaneous tissue, and galea from a pivot point until they reach the area of the defect that needs repair.[4]
Rotation flaps provide the ability to mobilize large areas of tissue with a wide vascular base for reconstruction. The name rotation flap refers to the vector of motion of the flap, which is curved or rotational, and the procedure involving these flaps can be thought of as the closure of a triangular defect by rotating adjacent skin around a rotation point into the defect. These flaps are advantageous because they have a particularly wide base and thus an excellent blood supply.[3]
However, when single rotation flap is performed for large defects, the arc length of the flap has to be extended to rotate the flap into the defect, resulting in narrower base and compromise blood supply to the graft and also higher degree of rotation can result in disorientation of hair direction. This can be prevented by increasing the number of flaps raised around the defect so that the length of arc can be minimum, thus maintaining vascularity. The main advantages of this double and triple rotation techniques are the natural appearance of the final result due to preservation of hair orientation, and the uniform distribution of the wound-closure tension over a wide peripheral area of the scalp, although extensive undermining is generally required.[35]
In the present case, similar technique was used to correct a medium-sized scalp defect. After excising the defect, three flaps were raised and rotated into the defect and closed in a fan-shaped pattern with well-maintained orientation of hair follicles so that the scar can be hidden by growing hair [Figure 5].

- Scar with well-oriented hairs that will cover once they are grown (hairs being trimmed to make scar visible)
The disadvantage of these techniques is that they require relatively extensive cutting beyond the defect to develop the flap, thus increasing the risk of nerve damage or bleeding. Complications can be prevented by the use of tumescent anesthesia, careful dissection, proper hemostasis, and pressure dressing.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflict of interest
There are no conflicts of interest.
REFERENCES
- Reconstruction of large scalp and forehead defects following tumor resection: Personal strategy and experience—analysis of 25 cases. Rev Bras Cir Plast. 2012;27:227-37.
- [Google Scholar]
- Local flap reconstruction of large scalp defects. Med Oral Patol Oral Cir Bucal. 2008;13:E666-70.
- [Google Scholar]
- The triple rotation scalp flap revisited: A case of reconstruction of cicatricial pressure alopecia. Int J Oral Maxillofac Surg. 2006;35:1153-5.
- [Google Scholar]
- Double-opposing unilobar rotation flaps in the reconstruction of moderate-to-large defects of the scalp. J Craniofac Surg. 2015;26:e523-5.
- [Google Scholar]




