
Translate this page into:
Tissue expansion and follicular unit extraction hair restoration in rehabilitation of a severe postburn deformity of neck and beard region

*Corresponding author: Satyaswarup Tripathy, Department of Plastic Surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India. dr.sstripathy@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kaushik R, Kalia D, Tripathy S, Sharma RK. Tissue expansion and follicular unit extraction hair restoration in rehabilitation of a severe postburn deformity of neck and beard region. J Cutan Aesthet Surg. doi: 10.25259/jcas_129_21
Abstract
Thermal burns of the face and neck remain one of the most common accidental injuries in young adults. This leads to various sequelae including scar, contracture, and alopecia. The goal of management is to achieve a complete range of motion of neck movements and restore esthetic appearance. Many reconstructive options are available in the form of split skin grafts, tissue expanders, loco-regional flaps, free flaps, and hair transplantation. Here, we report a case of severe postburn neck contracture and beard alopecia as sequelae of accidental thermal burns sustained by him 2 years back. The patient was successfully managed with contracture release followed by an expanded neck flap for coverage of the resultant defect. We also present the outcome and follow-up of the patient, after receiving follicular unit extraction from the scalp and contra-lateral un-burnt beard region for treatment of patchy postburn alopecia over the burnt beard area of the face. The quality of facial scarred skin has improved dramatically following the hair transplant which was proven by the punch biopsies obtained from the treated skin.
Keywords
Post-burn alopecia
Tissue expansion
Hair transplant

INTRODUCTION
Burn injury in the head and neck region has far-reaching consequences as compared to burns anywhere else in the body. Once acute management of facial and neck burns is completed, functional restoration and subsequent esthetic concerns must be addressed. Functional problems occur such as eyelid contractures, microstomia, ear deformities, neck contracture, and lip ectropion. Surgical release of contractures and resurfacing with split skin grafts, local flaps, and expanded flaps are available options. Full-thickness burns can cause complete loss of the hair follicular units leading to alopecia. The deep dermal burns if left alone heal by hypertrophic scarring with interspersed areas of alopecia due to follicular damage. Burns over the neck greatly affect the self-identity. They impair social and interpersonal relationships due to facial disfigurement. Management of alopecia in such scarred regions with hair transplantation is even more challenging. Surgical techniques outweigh all non-surgical methods in addressing alopecia of eyebrow, mustache, sideburn, and beard regions.1-3 We present management of severely scarred face and neck burns using expanded neck flaps and hair restoration using the follicular unit extraction (FUE) method.
CASE REPORT
A 25-year-old man presented to the Plastic Surgery Department in a tertiary care hospital with postburn contracture over his neck and alopecia patches over his lower face. He sustained an accidental burn about 2 years ago which was managed with dressings alone at a local facility [Figure 1]. This resulted in hypertrophic scar leading to Grade 3 Neck contracture (McCauley grading). Contracture release, excision of hypertrophic scar, and coverage with split-thickness skin graft were done. Neck extension just beyond neutral was achieved intraoperatively. The patient was kept on strict immobilization with a neck collar and aggressive physiotherapy thereafter. However, due to low compliance, he again started developing scarring over the neck [Figure 2]. Three years later, due to the recurrence of grade 3 neck contracture, the patient was planned for expander placement and neck flap re-draping. A rectangular expander of 11 × 6 × 6.2 cm was placed bilaterally. Serial expansion continued till the filling of normal saline up to the volume of 308 cc on the right and 268 cc on the left side, respectively [Figure 3]. Expanded flaps were re-draped [Figure 4]. Simultaneously lip ectropion was released and covered with a full full-thickness skin graft. Midline scar contracture developed in subsequent months, which was managed with multiple Z-plasty. The patient sought further treatment for beard alopecia for which he undertook treatment at a local private clinic. He underwent FUE from the occipital scalp and transplanted over the alopecic site at the beard region [Figure 5]. After undergoing two sessions of FUE, he underwent FUE from the contralateral normal beard region [Figure 6]. In subsequent follow-up, the patient achieved satisfactory results and was able to resume full occupational and social obligations [Figure 7]. The quality of the scarred skin has improved dramatically following the hair transplant. It has become soft, supple, and smooth. We have taken a small punch biopsy to demonstrate the improvement in the scarred skin over the face which showed near normal pilosebaceous units and improvement in the arrangement of the collagen bundles of the old scar [Figure 8].

- Postburn neck contracture at the time of presentation.

- Recurrence of postburn neck contracture after 3 years.

- Expander placement in bilateral neck and serial expansion.

- Expanded flap redraping with midline neck contracture.

- Multiple Z plasty for breaking midline scar and the first stage of hair restoration follicular unit extraction.
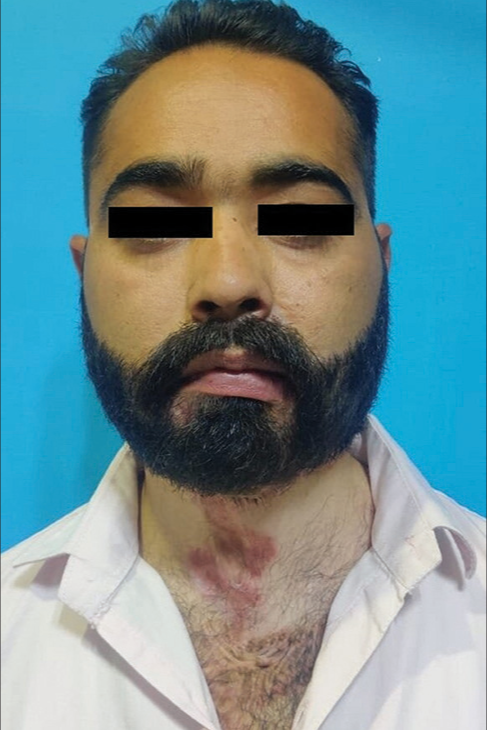
- After two stages of hair restoration.

- Patient attending a marriage ceremony recently.
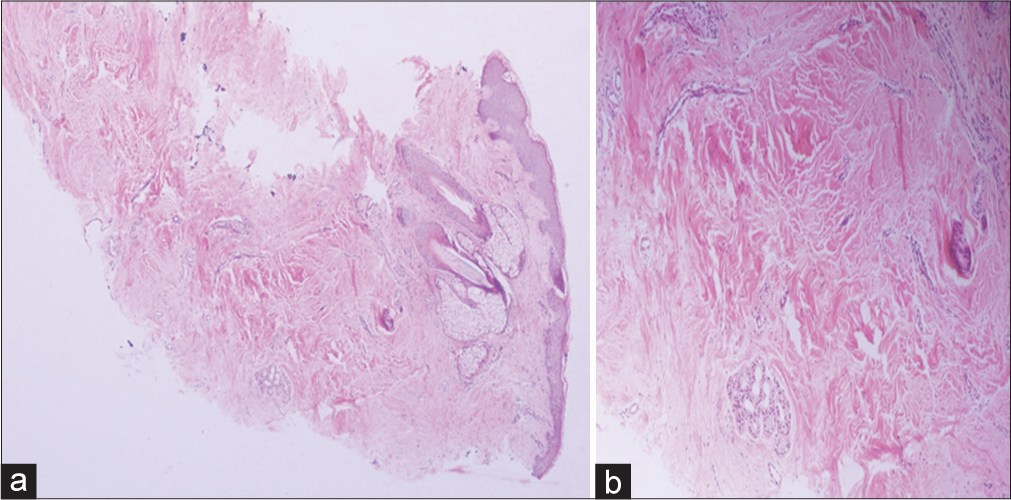
- (a) Punch biopsy of the left cheek alopecia where follicular unit extraction was done. Histological slide stained in hematoxylin and eosin stains in ×22.5 magnification showing pilosebaceous glands with hair shaft and hair follicles. (b) Minimal mononuclear infiltrate was seen in the dermis with haphazardly arranged collagen bundles suggesting an old scar.
DISCUSSION
Face plays an important role in social, interpersonal interactions and essential physiological functions. Extensive facial and neck burns pose a reconstructive challenge to surgeons. Due to the location of postburn scar and alopecia in this region, it is difficult to camouflage leading to severe psychological trauma.4 Reconstructive goals in neck contracture are to restore form, function, and esthesis. Early excision, grafting, and aggressive post-operative physiotherapy are the key to successful results in such cases. However, if the patient presents in a secondary setting with a matured scar and neck contracture, the primary focus is on the surgical release of contracture. Contracture release is followed by resurfacing with an intermediate-thickness skin graft. Tissue expansion is also indicated when other methods fail to cause satisfactory functional and esthetic outcomes. An expander can be placed in nearby intact skin in the supraclavicular or submandibular region in the subcutaneous plane. Advantages of expansion include replacement of like with like tissue, availability of large amounts of tissue aiding primary closure of donor site, reduction of alopecic defect, and a cover which is sensate.5
In a study by Fauerbach et al. in 2000, a greater amount of dissatisfaction outcomes were observed in adult head-and-neck burn survivors than non–head-and-neck burn survivors. This is due to disfiguring scars which took a longer time to mature before any surgical intervention could be done. Higher demands for reconstructive interventions such as scar revisions, local flaps, hair restoration, and lasers have been reported in patients with facial and neck postburn contractures.6
Burn alopecia can be managed with a multi-modal treatment approach. Non-operative treatment options are – cosmetic camouflage, hair-bearing adhesive prosthesis, and micropigmentation tattooing techniques. Among surgical options – hair restoration by hair-bearing flaps with or without tissue expansion or hair transplantation are available. As hair density is limited at the time of a single hair transplant procedure, it has been advised to proceed with the reduction of the alopecic defect by serial excision, tissue expansion, and hair-bearing flaps. Most of the time, multiple hair restoration procedures are done to create good-density hair and also replace lost grafts.7 E ach f ollicular u nit h as t he p otential t o survive in areas of fibrosis, burn s cars, and grafted skin. This is due to the lower metabolic requirement of hair grafts t o thrive in these areas.8 Following hair transplant in this case the scarred skin becomes soft and pinchable. Our study is unique as it demonstrates the improvement of the quality of the scarred skin following the hair transplant procedure in the alopecic areas. It is probably due to the placement of pilosebaceous glands in a scarred bed which proved beneficial in our case.
CONCLUSION
The procedure involving hair restoration by follicular unit extraction over an expanded flap can be performed to successfully manage the postburn scar and alopecia sustained after thermal injury over lower face and neck area. These procedures are effective in restoring function as well as aesthetic appearance for postburn sequeles in such regions.
Authors’ contributions
All the authors contributed to the research study. Tripathy Satyaswarup: conceptualization of idea of case report. Ritwik Kaushik and Deepak Kalia: Case Report Draft. T ripathy Satyaswarup and RK. Sharma: Supervision.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Hair transplantation in burn scar alopecia. Scars Burn Heal. 2015;1
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of quality-of-life in patients with face-and-neck burns: The Burn-Specific Health Scale for Face and Neck (BSHS-FN) Burns. 2018;44:1602-9.
- [CrossRef] [PubMed] [Google Scholar]
- Application of the expanded neck flap for face and ear reconstruction in burn patients: A report on 2 cases. Ear Nose Throat J. 2022;101:449-53.
- [CrossRef] [PubMed] [Google Scholar]
- Head and neck burns are associated with long-term patient-reported dissatisfaction with appearance: A Burn Model System National Database study. Burns. 2019;45:293-302.
- [CrossRef] [PubMed] [Google Scholar]
- Reconstruction of skin defects on the mid and lower face using expanded flap in the neck. J Craniofac Surg. 2017;28:e137-41.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of early body image dissatisfaction on subsequent psychological and physical adjustment after disfiguring injury. Psychosom Med. 2000;62:576-82.
- [CrossRef] [PubMed] [Google Scholar]
- Postburns hair restoration of eyebrow, eyelash, moustache, beard and scalp areas. Indian J Burns. 2015;23:26.
- [CrossRef] [Google Scholar]
- The use of micrografts and minigrafts in the aesthetic reconstruction of the face and scalp. Plast Reconstruct Surg. 2003;112:883-90.
- [CrossRef] [PubMed] [Google Scholar]




