
Translate this page into:
Tunneled Flaps: An Ingenious Reconstructive Option for Anterior Auricle Defects
Address for correspondence: Dr. Diogo Cerejeira, Rua Marta Mesquita da Câmara, nº110, A3 4ºDto – 4150-485 Porto, Portugal. E-mail: Diogo_cerejeira@hotmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Abstract
Background:
The anterior surface of the auricle is especially susceptible to a variety of traumatic insults and cutaneous malignancies. However, given the unique anatomy of this structure and the lack of local tissue available, the reconstruction of these defects is still a challenge. Despite of their positive outcomes, tunneled flaps have not been thoroughly explored in the literature.
Objectives:
To review the clinical utility of tunneled flaps in reconstructing anterior auricle defects.
Materials and methods:
A review of the literature on surgical reconstruction of the anterior auricle surface was performed in PubMed, with specific reference to tunneled flaps.
Conclusions:
When designed and executed properly, tunneled flaps offer unrivalled opportunities to reconstruct anterior auricle defects, with maximal preservation of the symmetry.
Keywords
Auricle reconstruction
postauricular “Revolving door” Island pedicle flap
postauricular pull-through transposition flap
tunneled flaps
tunneled postauricular advancement flap
tunneled preauricular transposition flap

INTRODUCTION
Reconstruction of the auricle is often a challenging yet rewarding procedure. The integrity of all components of the auricle, namely helix, scapha, antihelix, concha, triangular fossa, tragus, antitragus, and lobule, is important for both functional and aesthetic reasons.[12] Other items to be considered include its general oval contour, vertical position, protrusion, long-axis orientation, size, and discrete definition.[3] Suboptimal reconstructions can leave a patient with a striking asymmetry and poor functional results.
Because of its exposure, the anterior aspect of the auricle is especially susceptible to a variety of traumatic insults and cutaneous malignancies induced by actinic injury. When selecting the method of auricular reconstruction, the surgeon should make note of surrounding anatomic landmarks and the impact the surgery can have on them.[3] Composed by a tightly adherent skin over a cartilaginous framework, the anterior aspect of the auricle poses unique limitations regarding possible reconstructive options. Therefore, interpolated and tunneled flaps have been used in the auricle reconstruction, particularly when alternative repair options would introduce unacceptable anatomic distortion.
If properly executed, a tunneled flap offers unrivaled advantages in anterior auricle reconstructive surgery: (1) it allows tissue mobilization into areas in which adjacent available tissue is limited, (2) avoids the disruption of auricle symmetry that would be inherently associated with reconstructive alternatives, and (3) enables single-stage execution, which reduces costs and patient morbidity of further procedures.
In this study, we revise the applicability of tunneled flaps for the reconstruction of anterior auricle defects.
GENERAL PREPARATION
Before performing a tunneled flap, it is important to determine whether the defect can be appropriately repaired with a simpler alternative. If it cannot, then tunneled flaps can be considered to reconstruct the aesthetic units of the anterior auricle. All flap procedures are suitable to be performed under local anesthesia (2% lidocaine with epinephrine 1:100,000) using the sterile surgical technique. Subsequently, flaps are peripherally excised and undermined, paying special attention to preserving central or peripheral pedicles, and underlying anatomic structures. Once pedicle dissection is completed, the flaps are tunneled into primary surgical defects, where they are sutured to adjacent tissue. However, it is critical to ensure that the flaps and the pedicles are of the appropriate length to compensate for its tunneling. Equally important is the creation of a tunnel suitable for the width and thickness of the flaps. To enable a single-stage execution, the portion of the flaps beneath the tunnel must also be deepithelialized. Donor sites are usually primarily closed and sutures are removed 7–14 days after the surgical procedures.
ILLUSTRATIVE CASE EXAMPLES
Tunneled preauricular transposition flap
Although it was first described by Pennisi et al.[4] for earlobe reconstruction,[45] a tunneled preauricular transposition flap has also been used to repair partial-thickness surgical defects that involve triangular fossa, antihelix, concha, and antitragus. Depending on the inclusion of a superficial temporal artery perforator, this flap can be categorized either as an axial or a random flap. The possibility to be based superiorly or inferiorly also contributes to its increased versatility.[6] An example that demonstrates the practical use of this flap can be seen in Figure 1, in which the final defect involved a region of the concha and antitragus. An inferiorly based flap was outlined along the hairless area of the preauricular region, and dissected from the distal margin, above the superficial temporal vessels. The flap was then proximally de-epithelialized and a tunnel was created at the intertragal notch. Finally, the flap was transposed through the tunnel and laid atop the defect. Donor site was primarily closed with minimal cosmetic impact.
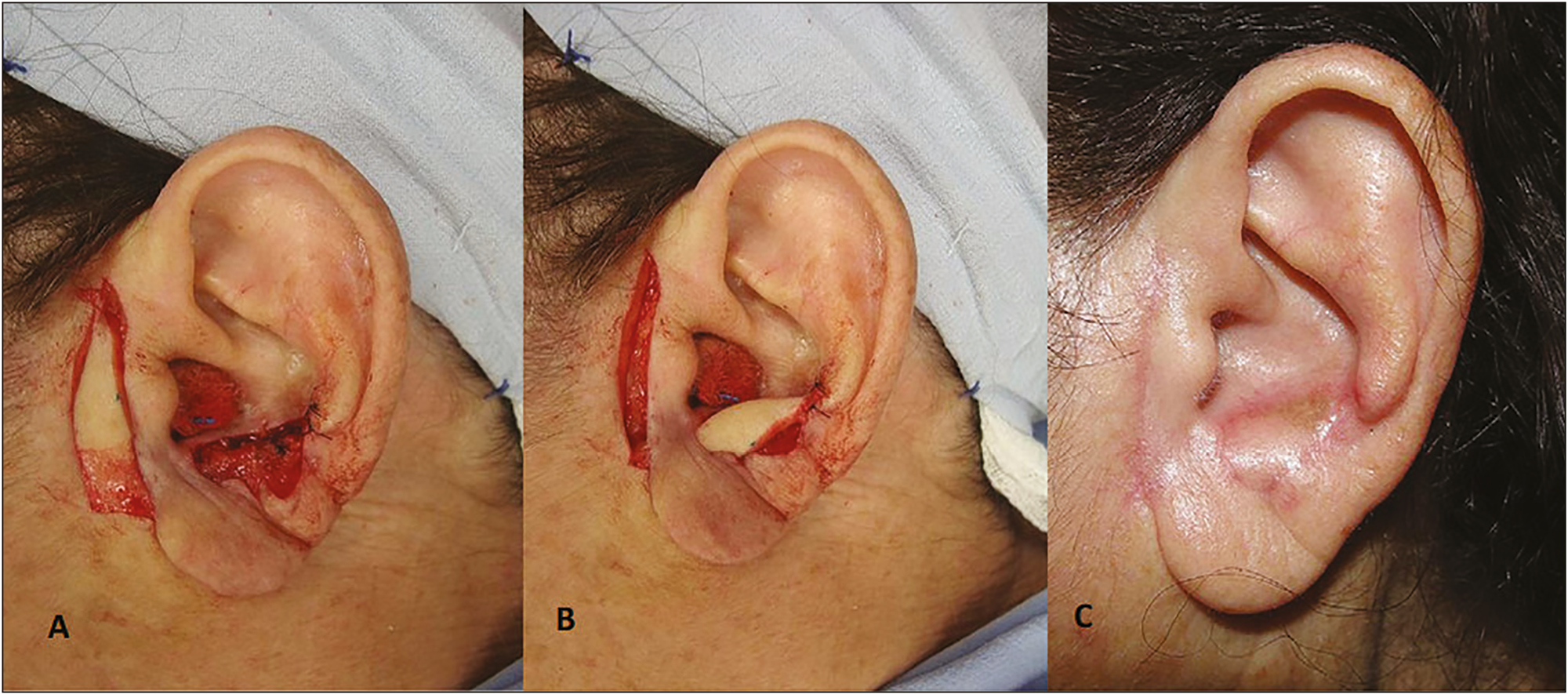
- Final defect involving a region of the concha and antitragus. An inferior-based preauricular flap was raised (A) and tunnelized into place (B). One-month postoperative photograph (C) (Courtesy of A. Braga)
Postauricular pull-through transposition flap
Postauricular pull-through transposition flap is a versatile reconstructive option that has been applied to defects of the scaphoid fossa, antihelix, and conchal bowl. Apart from being performed as a one-stage procedure, the flap’s main advantages are the possibility to cover large defects and the usage of a well-protected and vascularized skin.[7] When performing this procedure, the auricle is reflected anteriorly, and the flap is outlined just posterior to the postauricular sulcus. This flap is then peripherally excised and meticulously undermined, preserving a subcutaneous pedicle that originates from the postauricular sulcus. Returning the auricle to its normal anatomical position, a tunnel is created connecting the base of flap’s pedicle to the medial margin of the defect. Ultimately, the flap is pulled and adapted to the defect, without tension, torsion, or impingement of the pedicle. Figure 2 shows the usage of this flap in an antitragus defect reconstruction.
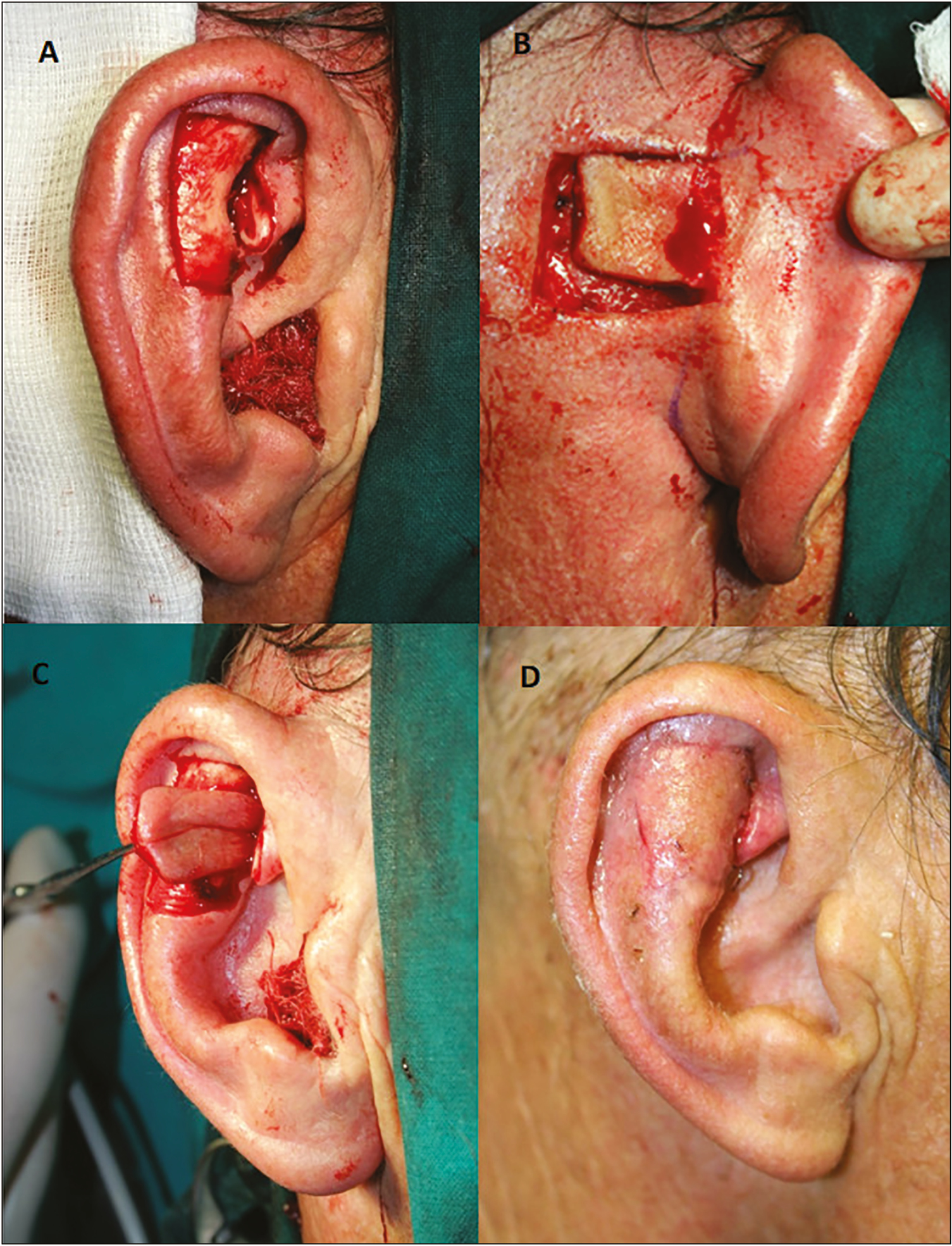
- Large triangular fossa defect shown after a squamous cell carcinoma excision (A). The flap was dissected in ipsilateral postauricular region (B) and mobilized through a cartilaginous tunnel (C) toward the defect. Three-week postoperative photograph (D)
Tunneled postauricular advancement flap
Advancement flaps are commonly used in auricle reconstruction as the postauricular skin can be easily dissected and anteriorly mobilized. Due to the presence of incorporated branches from the posterior auricular artery, these flaps are also richly vascularized and have a low complication rate associated with.[8] Traditionally, the tunneled postauricular advancement flap is elevated from the mastoid bone, conserving a posterior pedicle with the same width of the defect. An appropriate tunnel is then conceived in the auricle cartilage, connecting primary, and secondary surgical defects. The tunneled portion of the flap is superficially deepithelialized and the flap is advanced through the tunnel for anterior auricle reconstruction. Donor site is primarily closed and hidden in the postauricular sulcus. Although it is suitable to repair conchal and antitragus isolated defects [Figure 3], this flap may also be bivalved and used to repair more than one aesthetic unit.[9]
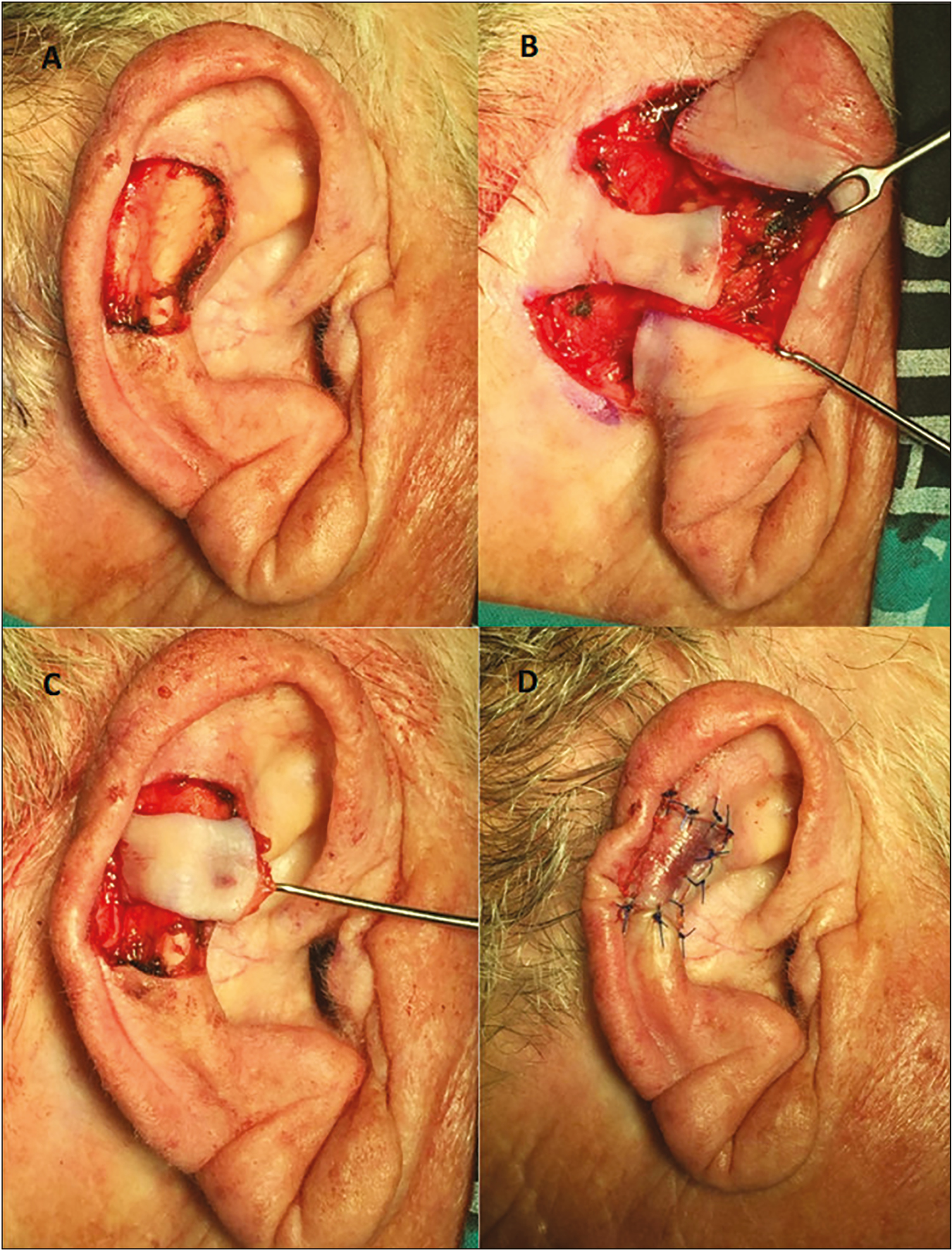
- The excision of a squamous cell carcinoma resulted in a defect of the scaphoid fossa (A). A posterior based flap was elevated in the postauricular region (B) and advanced through an auricle tunnel into the defect (C). Flap sutured into place (D)
Postauricular “revolving door” island pedicle flap
First described by Masson[10] and subsequently refined by Talmi et al.[11] and Redondo et al.,[12] this postauricular island flap is a versatile single-stage reconstructive option for medium to large defects of the scaphoid fossa, antihelix and conchal bowl.[7] Also known as the “flip flop” flap, this technique is shown in Figure 4, where the primary surgical defect included the skin and the underlying cartilage of the concha and external auditory meatus. According to the shape and size of the defect, a proper flap was designed in the posterior aspect of the auricle and mastoid region. The flap was then peripherally incised and undermined as an island, preserving a superior and inferior subcutaneous pedicle at the postauricular sulcus. With a skin hook, the most distal margin of the flap was pulled through the conchal defect and was sutured to the most medial margin of it. The periphery of the flap was sutured in place and the donor defect was primarily closed.

- Illustration of a conchal bowl defect after a wide excision of a basal cell carcinoma (cartilage removed with the tumor) (A). Design of the flap in the postauricular and mastoid region (B). Flap dissection preserving a superior and inferior subcutaneous pedicle (C). The flap was pulled through the conchal defect (D) and sutured in place (E). Two-month postoperative photograph (F)
DISCUSSION
Malignant lesions of the external ear account for approximately 6% of all head and neck skin cancers.[13] The excision of these tumors and other eventual injuries results in a wide heterogeneity of defects, varying in size, shape, and deepness. Several procedures have been described for reconstructing the anterior auricle surface. Unfortunately, most of these reconstructive options are associated with significant drawbacks and may result in unfavorable functional and cosmetic outcomes.
Primary surgical repair is rarely used due to the peculiar anatomy of the auricle. Second intention healing, although is ideal for small, shallow defects of concave surfaces (such as the scaphoid fossa and conchal bowl), results in unpredictable scars and in an increased risk of cartilage infection. In addition, it requires a long healing process, which can be unpleasant for the patient. Skin grafts may also be considered. However, the viability of the graft on bare cartilage may require excision or perforation of the cartilage to conceive imbibition and inosculation from the opposing perichondrium.[7] The removal of the cartilage, which is important for structural support of the ear, can cause some degree of distortion and contracture of the skin graft. Moreover, the aesthetic results are inferior to those for local flaps, owing to the poorer color and texture match of the skin graft. Numerous local flaps were used, many of them being interpolated and requiring two surgical stages.[2] Furthermore, some traditional local flaps may cause asymmetries and often require a cartilage graft, which can be associated with an increased operative time and donor site morbidity.[6]
The main advantage of tunneled flaps over other reconstructive techniques is their ability to be transposed across anatomic boundaries and repair deep, complex defects in a single-stage procedure. This ingenious idea of passing a flap through a cartilaginous tunnel is especially useful in preserving the overall architecture of the auricle, as its reconstruction does not involve any other auricle subunit. If properly executed, these flaps are also capable of disguising donor site scars and provide an excellent color and texture match, conferring excellent cosmetic results. Additional benefits include their reliable vascular supply and the obviation of cartilage grafts.
Tunneled flaps are, however, time-consuming and require some surgical expertise. Pedicle dissection must be careful and should compensate for the shortening caused while mobilizing the flap. Also, the incision of auricular cartilage must be suitable to the pedicle tunnelization. Over manipulation of auricular cartilage may lead to pain and chondritis.[7]
CONCLUSION
Given their potential advantages, tunneled flaps are a versatile reconstructive choice for anterior auricle defects and an excellent addition to the surgeon’s armamentarium.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Tunnelized preauricular transposition flap for reconstruction of auricular defect. J Dermatolog Treat. 2014;25:441-3.
- [Google Scholar]
- Tunnelised inferiorly based preauricular flap repair of antitragus and concha after basal cell carcinoma excision: case report. J Plast Reconstr Aesthet Surg. 2011;64:e73-5.
- [Google Scholar]
- Cadaveric dissection and clinical experience with 20 consecutive tunneled pedicled superficial temporal artery perforator (STAP) flaps for ear reconstruction. Microsurgery. 2015;35:190-5.
- [Google Scholar]
- Pull-through subcutaneous pedicle flap for an anterior auricular defect. Dermatol Surg. 2010;36:945-9.
- [Google Scholar]
- The postauricular cutaneous advancement flap for repairing ear rim defects. Dermatol Surg. 1996;22:28-31.
- [Google Scholar]
- A simple island flap for reconstruction of concha-helix defects. Br J Plast Surg. 1972;25:399-403.
- [Google Scholar]
- Auricular reconstruction with a postauricular myocutaneous island flap: Flip-flop flap. Plast Reconstr Surg. 1996;98:1191-9.
- [Google Scholar]
- Aggressive tumors of the concha: Treatment with postauricular island pedicle flap. J Cutan Med Surg. 2003;7:339-43.
- [Google Scholar]
- Aesthetic reconstruction of the upper antihelix in external ear with banner pull-through flap. J Cutan Aesthet Surg. 2015;8:218-21.
- [Google Scholar]




